The New York State workers compensation board has developed these guidelines to help physicians, podiatrists, and other healthcare professionals provide appropriate treatment for Guidelines for Optimizing Opioid Treatment.
These Workers Compensation Board guidelines are intended to assist healthcare professionals in making decisions regarding the appropriate level of care for their patients with ankle and foot disorders.
The guidelines are not a substitute for clinical judgement or professional experience. The ultimate decision regarding care must be made by the patient in consultation with his or her healthcare provider.
Guidelines for Optimizing Opioid Treatment of Pharmacological Approaches
Introduction of Optimizing Opioid Treatment
Patients on persistent narcotic treatment need customary observing and re-assessment to measure patient adherence and progress towards treatment objectives, with documentation in the clinical record at every patient visit.
The Aggravation Evaluation and Documentation Device (PADT) is a compelling methodology for methodically recording each experience and helping with coordinating the administration and audit of care. (See Informative supplement C)
Assessing Effects of Long-Term Opioid Therapy
The doctor ought to evaluate/re-survey dangers and advantages of the patient’s current narcotic treatment including:
- Capability and agony status.
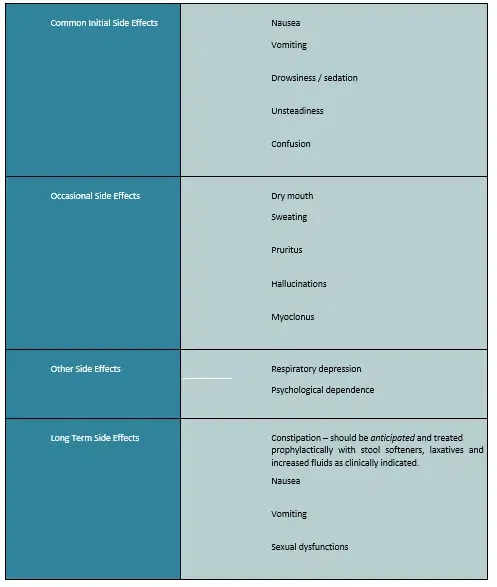
- Conceivable unfavorable impacts of current narcotic portions (See Table 3: Unfavorable Impacts of Narcotics).
- Period of Patient (old).
- Potential mental problems influencing treatment.
- Potential circumstances that might potentiate narcotic unfriendly impacts like COPD, CHF, rest apnea, or history of renal/hepatic brokenness (counting recently analyzed conditions and related drugs).
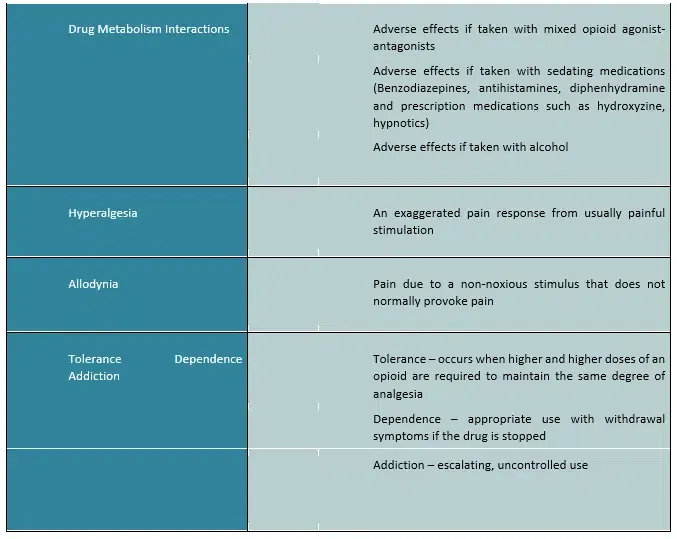
- Conceivable medication blends that might potentiate narcotic unfavorable impacts like narcotic hypnotics, benzodiazepines, or barbiturates except if there is a particular clinical as well as mental sign for the mix (what’s more, expanded checking is performed).
On the off chance that there is proof of huge unfavorable impacts from narcotic treatment, the doctor ought to diminish the narcotic portion and reevaluate the patient’s status.
- Tightening/cessation of narcotics might be essential because of the advancement of resistance, hyperalgesia, diminished impacts from a narcotic, absence of consistence with the narcotic agreement or intolerable incidental effects.
- Long term treatment might be expected for enslavement or narcotic tightening in complex cases.
Table 3: Adverse Effects of Opioids
If the patient shows improvement from the opioid therapy (supported by validated measures of improved function and pain), maintenance of opioids may be reasonable if there are no signs for dose decrease or termination of opioids.
However, continued therapy necessitates continual assessment and monitoring. The patient’s mental acuity, alertness, and capacity to engage in work tasks safely while receiving continuing opioid medication may now be evaluated by the treating physician. Unless there is a clear functional benefit,
When mental acuity or alertness is compromised as a result of opioid therapy, the patient shouldn’t engage in safety-sensitive activities or activities that could endanger personal, professional, or public safety.
Operating powered vehicles, working at heights or in restricted places, using machinery that could result in significant damage if used improperly, and operating power tools are just a few examples of such activities.
Patient Informed Consent for Opioid Treatment Form and Patient Understanding for Opioid Treatment Form
Patient Informed Consent for Opioid Treatment Form (Appendix F) contains the following:
- Possible secondary effects from the prescription including yet not restricted to disarray/obfuscated judgment, queasiness, stoppage, retching, tiredness/sleepiness, issues with coordination, balance, and diminished response time, breathing too leisurely (counting probability that breathing can pause and prompt passing), exacerbation of misery, and dry mouth.
- Hyperalgesia. In certain patients, an expanded portion of narcotics might diminish torment edge and increase aversion to torment. Side effects frequently improve with decline in the narcotic portion.
- Secondary effects might be more regrettable assuming narcotics are blended in with different medications, including liquor.
- Chances, resistance, reliance, and fixation.
- Guys. Low testosterone levels (may influence sexual want and sexual execution).
- Females. Pregnancy while taking narcotics, potential reliance of infant.
Patient Understanding for Opioid Treatment Form (Appendix G) contains the following:
- Patient consents to take meds at measurements and recurrence as endorsed and acquire medicine at one drug store.
- Meds will be acquired from the doctor (or NP/Dad) who signs the structure, or during his/her nonattendance, by the covering doctor (or NP/Dad).
- Necessity to proceed with dynamic treatment.
- Comprehension of the need to seek after other agony the executives’ strategies to work with nonacute torment.
- Treatment objectives which should remember improvement for agony and capability including return to work in general cases.
- Need to stay away from liquor and different medications that are not part of the treatment plan.
- Assumption for UDT and blood tests and outcomes of surprising outcomes, including a conversation with respect to how evaluates positive for nonprescribed medications or liquor will be taken care of.
- Explanations behind the end of narcotic administration (e.g., rebelliousness, redirection).
- Purposes behind tightening or end of narcotics (e.g., need of progress toward helpful objectives, insufferable side impacts): if a narcotic preliminary or treatment fizzles, tightening or end is normally finished north of 30 days or by reference for habit treatment.
- Safe capacity of drugs.
Urine Drug Testing (UDT) for Monitoring Opioid Therapy
UDT Introduction
The reason for drug testing is to distinguish deviant ways of behaving, undisclosed drug use and additionally misuse, and check consistency with treatment. When utilized with the suitable degree of understanding, UDT can work on the doctor’s capacity to oversee narcotic treatment securely and suitably.
Irregular UDT is prescribed as an instrument to screen consistency with endorsed substances, as well as distinguish utilization of undisclosed substances which will influence treatment choices.
- Urine Medication Testing is a compulsory part of persistent narcotic administration, as a component of the gauge evaluation, furthermore, progressing re-evaluation of narcotic treatment. (See Table 4: Urine Medication Testing (UDT) Dangers and Recurrence of Testing)
- Pattern UDT ought to be acquired on all moving patients who are now utilizing narcotics or when a patient is being considered for progressing narcotic treatment.
Table 4: Urine Drug Testing (UDT) Risks and Frequency of Testing
- Before testing, the doctor ought to illuminate the patient regarding the justification for the testing, the assumption for future testing (which might be unscheduled) to show adherence with the Patient Comprehension for Narcotic Treatment Structure, and the outcomes of unforeseen outcomes.
- Doctors should rehash UDT haphazardly based on understanding’s gamble classification (See Table 2: Narcotic Gamble Apparatus [ORT] and Table 4 above.
- Directing UDTs with a recurrence more prominent than those suggested in Table 4 ought to incorporate an enunciated clinical legitimization for the expanded recurrence by the requesting Provider.
- The medications tried for in the UDT are not set in stone on a case explicit premise in view of the clinical judgement of the requesting doctor. If exorbitantly huge test boards are requested, doctors will be requested to make sense of their clinical reasoning.
- If a patient exhibits a variant way of behaving (e.g., lost remedies, different solicitations for early requests, narcotics from various doctors, unapproved portion heightening, clear inebriation, and so on), doctors will test at that visit.
Confidentiality and Reporting UDT Result
- The patient has the option to reject a urine drug test. The patient will not get the narcotic medicine because of the refusal. Solution of narcotic agony drugs remains at the caution of the doctor through the clinical course of treatment.A patient’s refusal to take part in even a single UDT might be the reason for a provider’s choice to not start (or to suspend) narcotic treatment.
- UDT results are not to be delivered to the transporter, boss, or the Board. In any case, the treating doctor should confirm the patient’s adherence to or rebelliousness with the Patient Getting it for Narcotic Therapy Structure in the clinical record.Rebelliousness would incorporate (however not really be restricted to) proof that a patient is taking any non-recommended drug(s) or not consuming those medications recommended as a feature of treatment. Resistance can likewise be a refusal to go through UDT, as noted above.
- The recurrence of UDT depends on the clinical judgement of the treating doctor, applying the rules put forward thus (see Tables 2 and 4 above).Doctors need not feel a sense of urgency to perform UDTs if such demand is not in line with these rules.
- Employers can’t utilize test results to fire a worker in any biased or retaliatory way.
- The suggestions in the New York Clinical Treatment Rules don’t have any significant bearing to acute circumstances.
- Rule explicit measures will be utilized to decide when and at what recurrence UDT ought to be utilized.
Methods of Urine Drug Testing
Two primary sorts of UDT are accessible (see extra data, Supplement E: Medication Testing):
- Immunoassay drug testing (introductory medication test or screen)
- Is the most widely recognized strategy for testing.
- Beginning medication test or screen.
- Can be acted in a lab or office (at the place of-care).
- UDT can identify the presence or nonattendance of a medication or medication class, yet not the amount of a medication was utilized.
- Benefits of immunoassays are their capacity to simultaneously test for various medication classes, give quick outcomes and guide suitable use of corroborative testing.
- Immunoassays can respond with different medications and shift in awareness and explicitness.
- Surprising immunoassay results ought to be deciphered with alert and checked by corroborative testing.
- Office conventions and strategies ought to be created to guarantee a suitable assortment of drug tests.
- Superior execution chromatography/mass spectrometry (corroborative medication test)
- If a check or ID of a particular medication or potentially metabolite is required, then, at that point, corroborative testing is suggested.
- Lab based affirmation utilizes gas chromatography/mass spectrometry or fluid chromatography/pair mass spectrometry (GC/MS or LC/MS).
Interpreting Results
- Deciphering UDT results can be testing, particularly when the parent medication can be utilized to other ordinarily endorsed drugs.
- At the point when an immunoassay result is surprising, a corroborative test utilizing GC/MS or LC/MS ought to be requested.
Table 5: Red Flag Results

- Negative results:On the off chance that corroborative testing and clinical judgment validate a red banner (see Table 5: Warning Outcomes) and the outcome is negative for the endorsed opioid(s), the patient ought to be gotten back for a pill count and rehash test.On the off chance that this is still negative, the patient ought to get back to the workplace in two days and be assessed for proof of withdrawal. If no proof of withdrawal, consider halting opioid(s) as redirection is thought.
- Positive outcomes:
If corroborative testing and clinical judgment validate a red banner (See Table 5: Warning Outcomes) and the outcome is positive for a non-recommended planned drug or different medications without substantial clinical clarification, the supplier needs to comprehend the clinical meaning of this outcome.When an evaluation of the meaning of the positive drug test is made, choices like emphasis of the Patient Comprehension for Narcotic Treatment, weaning or end of narcotic solution, more continuous checking, reference to specialty care should be thought of, especially without a legitimate clarification.- Negligibly, in the setting of the over, a few activities ought to be stuck to, including (1) the harmed laborer is to be thought of “high gamble”, with testing recurrence to be reflected as portrayed for this new arrangement; (2) random pill counts are to happen on an occasional premise, quarterly
- In the event that there in this manner is a second certain drug test without legitimate clarification, e.g., finding a nonprescribed planned drug, finding of any medication without a substantial clinical clarification, or a deviation from expected prescription recurrence count.Then, at that point, prescription tightening is to quickly initiate, for a timeframe regularly not to surpass more than one month (except if obviously expressed clinical contraindications exist) or in a way as expressed somewhere else in this rule or its Supplements.
- As another option, a three to multi day long term therapeutically helped withdrawal (detox) program can be thought of, commonly under the management of a doctor who is suitably prepared and additionally board confirmed in fixation medication, and perhaps in combination with longer term support (e.g., Drunkards Unknown, Opiates Mysterious, bunch gatherings, office visits, and so forth), as shown.
- Note that any of the accompanying ought to likewise set off position of the patient to the “high-risk” classification: selling physician endorsed drugs, producing medicines, taking or acquiring drugs, every now and again losing solutions, forceful interest for narcotic prescription past sensible clinical boundaries, unsanctioned utilization of narcotic prescription, unsanctioned portion acceleration, getting narcotic prescription from numerous providers repeating Crisis Division visits for torment drug.
- Contact your neighborhood lab chief for help with deciphering drug testing results.
Optimizing Opioid Doses
- Utilize the most reduced conceivable powerful portion of narcotics and for opioid naïve patients, titrate gradually.
- Albeit logically higher dosages might further develop side effect control, rehashed portion accelerations can be a marker for misuse or redirection or can strangely initiate unusual agony awareness including hyperalgesia and allodynia.
- For patients taking more than one narcotic, the morphine comparable dosages (Drug) of the different narcotics should be added together to decide the aggregate portion.
- Narcotic turn (suspending a narcotic and changing to another) is a conceivable choice for patients who have insufficient side effect help despite of portion accelerations or who foster painful incidental effects.
- Notwithstanding, if the narcotic treatment is helping the patient as illustrated by true proportions of capability and torment, and not causing any perceivable antagonistic incidental effects, it very well might be fitting to proceed the portion while keeping up with proper thorough patient checking.
Equianalgesic Doses (ED)
Changes starting with one narcotic then onto the next are appraises for the most part considering equianalgesic dosing (see Table 6). Because of huge patient fluctuation considering narcotics.
Equianalgesic Doses (ED) are recommended – in the wake of working out the fitting transformation portion, the portion ought to be decreased by half to guarantee patient security.
- Narcotic withdrawal side effects are disagreeable yet not life undermining. Be that as it may, going too far is dangerous. Patients (family or companions) ought to be cautioned about indications of excess (slurred discourse, close to home lability, ataxia, falling asleep during discussion and additional action).
- It is more secure to underdose.
- Patient ought to be assessed not long after changing to a new narcotic to screen for agony and likely aftereffects.
- High portion or delayed use can result in narcotic actuated hyperalgesia.
Table 6: Oral Opioid Analgesic Equivalence (ED) to Oral Morphine 30mg
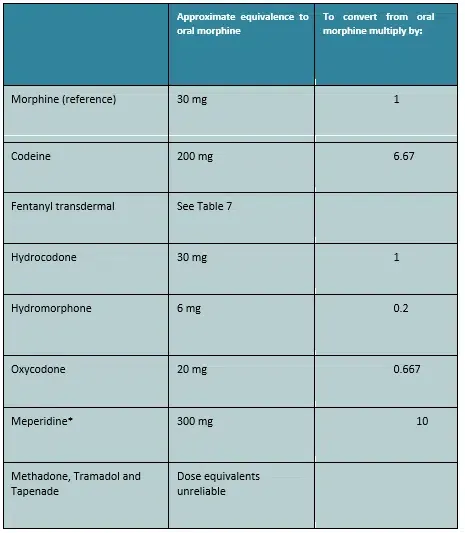
*The use of meperidine in the management of non-acute pain is not advised.
Table 7: Equivalence Between Oral Morphine and Transdermal Fentanyl (use only when converting from another opioid to fentanyl patch)
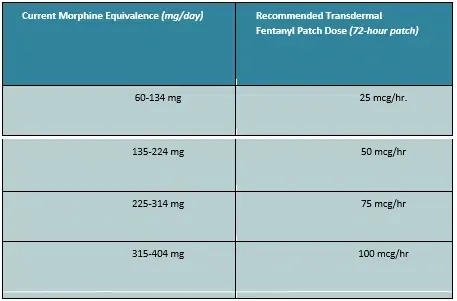
- Start fentanyl fix utilizing the suggested portion and titrate patients no more habitually than three days after the underlying portion and at regular intervals from there on until pain relieving adequacy is achieved.
- Change from fentanyl fix to another narcotic can misjudge the portion of the new specialist and may result in overdose.
- Most patients are sufficiently kept up with fentanyl fix managed like clockwork. A few patients may not accomplish satisfactory absence of pain utilizing this portion span and may require the fix to be applied at 48-hour spans. An expansion in the fix portion ought to be assessed to keep up with patients on a 72-hour routine, prior to endeavoring a change to a 48-hour portion stretch.
- Dosages of fentanyl fix over 25 mcg/hr. or spans more limited than 72 hours require either that the patient exhibits improvement in agony and capability without unusual way of behaving, or that an interview with either a torment the executives master or a doctor work in compulsion medication be gotten.
- Fentanyl Quick Delivery (Transmucosal) isn’t suggested.
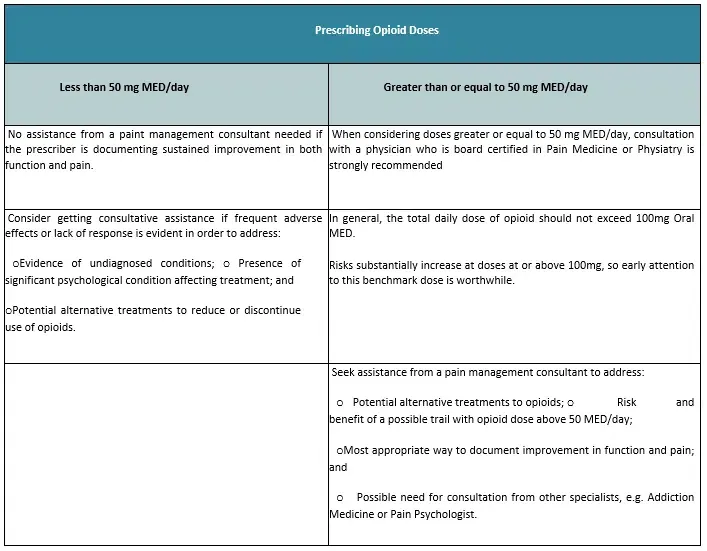
Opioid Doses greater than or equal to 100mg/MED
- As a rule, the all-out day to day portion of narcotic shouldn’t surpass 100 mg/oral Prescription and for longer term, low-portion treatment, the all-out day to day portion ought to for the most part not surpass 50 mg/oral Drug.
- Risk for glut or unfriendly impacts considerably increases at dosages > 100 mg/oral Drug.
- Apart from agony, the board or habit medication subject matter experts, a supplier shouldn’t recommend in excess of 100 Drug/day without either the patient exhibiting improvement in torment furthermore, capability without distorted conduct and without unfavorable secondary effects or first getting a conference from an aggravation the board trained professional or a doctor work in enslavement medication (see Table 8: Direction for Looking for Consultative Help).
- If dosing arrives at 100 mg/Drug/day and the patient has not gotten relief from discomfort or has created hyperalgesia, portion decrease, or suspension is justified.
- Relentless dosages > than 100mg/Prescription/day by any clinical supplier might be dependent upon an optional survey by an outer counsel in torment the board or compulsion medication.
- For patients taking more than one narcotic, the Prescription dosages of the different narcotics should be added together to decide the total portionA Prescription portion number cruncher is accessible at the opioid dose calculator.
- Washington State’s Prescription portion number cruncher ought to be not utilized to decide dosages when changing over a patient starting with one narcotic then onto the next. This is particularly significant for fentanyl and methadone changes. Equianalgesic portion proportions are as it were approximations and don’t represent hereditary elements, deficient cross-resistance, and pharmacokinetics.
Table 8: Guidance for Seeking Consultative Assistance
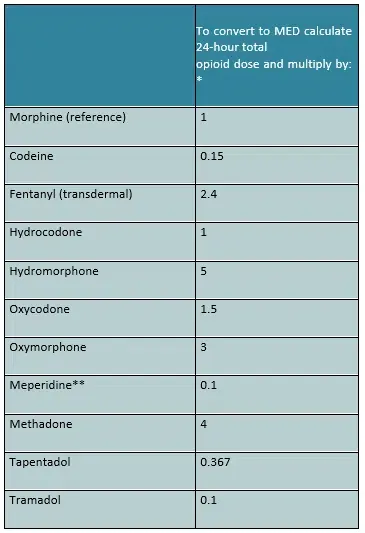
MED Dose Calculator (Opioid Analgesic Equivalence Ratio to Oral Morphine)
Table 9: MED Dose Calculator (Opioid Analgesic Equivalence Ratio to Oral Morphine)
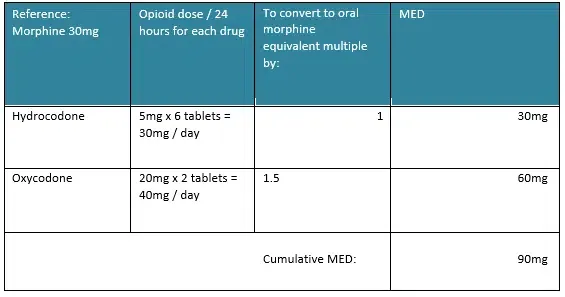
Example: Calculating Morphine Equivalent Dose (MED)
If a patient takes six hydrocodone 5 mg / acetaminophen 500 mg and two 20 mg oxycodone extended release tablets per day, the cumulative dose using Morphine 30 mg as the reference, may be calculated as follows:
- Hydrocodone 5 mg x 6 tablets per day = 30 mg per day.
- Oxycodone 20 mg x 2 tablets per day = 40 mg per day
- Cumulative dose is 30 mg + 60 mg = 90 mg morphine equivalents per day
Reasons to Discontinue Opioids and/or refer to a Physician specializing in Addiction Medicine or Pain Management:
- No improvement in capability and torment, or
- Narcotic treatment produces critical unfavourable outcomes (see Table 3: Unfriendly Impacts of Narcotics), or
- Patient displays abnormal way of behaving, drug chasing ways of behaving or redirections, for example,
- Selling physician endorsed drugs.
- Manufacturing solutions.
- Taking or acquiring drugs.
- Every now and again losing solutions.
- Forceful interest for narcotics.
- Unsanctioned utilization of narcotics.
- Unsanctioned medication heightening.
- Simultaneous utilization of illegal medications.
- Infusing oral/effective narcotics.
- Bombing drug screen (simultaneous utilization of liquor or non-endorsed drugs).
- Getting narcotic from different prescribers/drug stores.
- Missing arrangements.
- Not following different parts of the treatment plan (active recuperation, work out, and so forth.).
- Repeating crisis visits for acquiring extra torment prescription.
General Guidelines for Opioid Tapering/Discontinuation
For more point-by-point direction, if it’s not too much trouble, see Informative supplement H:
Definite Direction on Narcotic Tightening.
Medicinally, weaning from narcotics should be possible securely without huge wellbeing takes a chance by leisurely tightening the narcotic portion and considering the accompanying:
- A decline by 10% of the first portion each week is normally very much endured with negligible physiological antagonistic impacts.
- A few patients can be tightened more quickly (north of six to about two months) without issues.
- If a narcotic restraint condition is experienced, it is seldom therapeutically serious even though side effects might be unsavory.
- Side effects of forbearance disorder, like sickness, looseness of the bowels, muscle agony and myoclonus can be made do with clonidine 0.1-0.2 mg orally like clockwork or clonidine transdermal fix (0.1 mg/24 hours), with week-by-week assessments during the shape while checking frequently for huge hypotension and anticholinergic side impacts.
- In certain patients it might very well be important to slow the tighten timetable month to month, as opposed to week-by-week dose changes.
- Side effects of gentle narcotic withdrawal might endure for six months after narcotics have ceased.
- Fast re-event of resilience can happen for months or years after earlier ongoing use.
- Think about utilizing adjuvants, like antidepressants, to oversee irritability
- Try not to treat withdrawal side effects with narcotics or benzodiazepines in the wake of ending narcotics.
- Reference for advising or other help during this period is suggested if there are huge conduct issues.
- Reference to a doctor spending significant time in dependence medication or to an aggravation trained professional or potentially an ongoing/short term therapeutically helped detoxification program ought to be made for confounded withdrawal side effects.
Recognizing and Managing Behavioral Issues during Opioid Tapering
- Unique consideration should be taken to protect the patient-doctor remedial relationship during this time to abstain from accelerating specialist shopping, illegal medication uses or other hazardous patient ways of behaving.
- Very testing conduct issues might emerge during the time of a narcotic shape.
- Proper reference/meeting ought to be made. For model, self-destructive ideation with plan or goal ought to brief quick mental conference.
Specialty Consultations (See Table 8: Guidance for Seeking Consultative Assistance)
- Dependence/Agony Medication
- High gamble patients.
- Moderate gamble patients, reference or ecomanagement.
- Tightening/stopping of narcotics.
- Complex issues.
- Distorted drug ways of behaving.
- If more than two narcotics are being considered for long haul use, a second assessment from a trained professional who is Board Affirmed in
- Compulsion or Torment Medication is emphatically suggested.
- Narcotic doses > 100 mg/Drug/day (see Area F.3.e.ii), including Fentanyl (see Segment F.3.e.i)
- Methadone/buprenorphine treatment.
- Habit the executives.
- Psychiatry
- Decaying mental state (self-destructive ideation) during narcotic withdrawal.
- Side effects of temperament, nervousness, and insane messes.
- Undiscovered mental/mental messes.
- Other meeting to address instances of extreme agony with no improvement despite treatment with narcotics, including nervous system science, actual medication, muscular health, rheumatology, anesthesiology, oncology as clinically demonstrated by the patient’s signs and side effects,
- Interview ought to address conceivable undiscovered conditions, mental circumstances, and option treatment.
- Ongoing treatment might be expected for habit or narcotic tightening in complex cases.
What our office can do if you have workers compensation injuries
We have the experience to help you with their workers compensation injuries. We understand what you are going through and will meet your medical needs and follow the guidelines set by the New York State Workers Compensation Board.
We understand the importance of your workers compensation cases. Let us help you navigate through the maze of dealing with the workers compensation insurance company and your employer.
We understand that this is a stressful time for you and your family. If you would like to schedule an appointment, please contact us so we will do everything we can to make it as easy on you as possible.
