If you were injured your thumb and fingers at work and you are looking to see what is involved in “Scheduled Loss of Use” (SLU), you’re in the right place! You may be eligible for a compensation payment that is calculated according to the Workers’ Compensation Board’s standards.
Our report will state that because of your job-related injury, you have lost function in your thumb and hand that will never return. We follow Workers’ Compensation Guidelines for Determining Impairment. This post is based on New York state workers compensation guidelines.
We’ll go over how we evaluate you for SLU for your injured thumb and fingers.
Objectives for Determining Thumb and Finger Impairment
The objective is to precisely determine the long-term physical deficit that you experienced as a result of their accident. We will evaluate the damage as a result of a permanent physical impairment brought on by job accidents. The assessment is based on factual information gleaned from the history and physical examination, as well as any relevant diagnostic test results.
Techniques for Evaluating Permanent Impairment
When medical improvement has reached its limit and no further improvement is anticipated, it is necessary to assess the level of permanent residual physical impairment. Maximum medical improvement should be assessed in light of the clinical course of treatment’s results, the medical provider’s experience, and any additional treatment alternatives the patient may have. The consequent detrimental effect of injury to the hand may have substantial effect on the quality of life.
We take into account the contralateral extremity and expected/normal values when assessing the degree of permanent residual physical deficiency. The interval between an injury and the point of greatest medical progress can vary, although in most situations it is one year after the injury or the most recent surgery.
The mechanism of the damage has little bearing on how severe the permanent residual physical deficiency is. In addition to physical injury to bone, muscles, cartilage, tendons, nerves, blood vessels, and other tissues, it can also reflect the permanent residual physical deficit at the time of the maximum medical improvement.
Workers’ Compensation guidelines for Maximum Rating of Body Part
Workers’ Compensation guidelines are followed by us when assessing any permanent physical deficits in the thumb and fingers. The loss or impairment of a single digit must be assessed solely on the digit and not on the hand as a whole. If more than one joint is afflicted, the overall range of motion cannot be greater than the digit’s maximum value.
The overall impairment cannot be greater than 100% of the next largest significant member when multiple digit impairments are taken into account in a single comprehensive rating. Hence the loss of multiple digits, resulting in conversion to a hand impairment, may not exceed 100% schedule loss of the hand.
These pictures show the joints of the hand and their range of motion.

Joints of Thumb. IP is interphalangeal joint. MCP is Metacarpophaleangeal joint. CMC is carpometacarpal joint
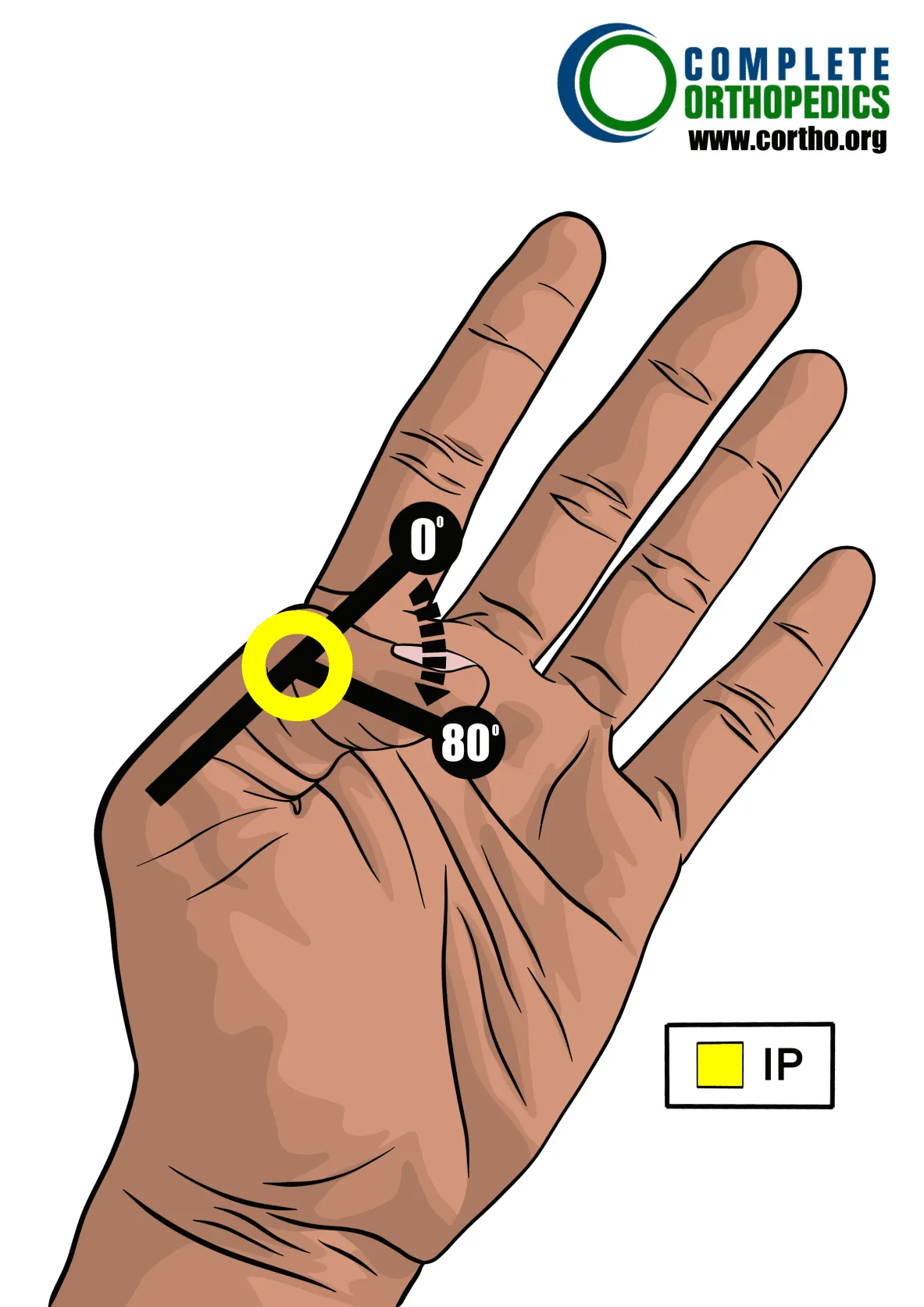
Degrees of motion of the interphaangeal joint (IP joint)

Degrees of motion of the Metacarpopalangeal joint (MCP Joint)
CMC Joint Position Measurement
The carpometacarpal joints of the fingers are synovial plane joints that act as the point of contact for the bases of the metacarpal bones and function as the articulation between the carpals and the metacarpals. There are a total of five CMC joints, with the thumb’s carpometacarpal joint being the most specialized and flexible.
Flexion/Adduction/Opposition of the fingers
The majority of the hand’s functions are carried out by these motions (flexion, adduction, and opposition). They enable pinching, prehension, and object manipulation by tip-to-tip contact.
Here’s how it’s measured:
The hand is held flat and facing up, the thumb rotates as it is extended as far over the palm as it can go. This is apparent as the thumbnail location varies. When more rotational degrees are applied in this action, the thumb tip contacts the MCP joints, making the change from full flexion to opposition obvious.
When there is complete opposition, the MCP of the pinky or little finger makes contact with the tip of the thumb (4th finger).
– The pinky’s MCP does not make touch with the tip of the thumb in a slight deficiency (1), but it does so with the ring finger’s MCP. In a medium deficiency (2), the MCP of the middle finger (2nd finger) makes contact with the tip of the thumb, but not the MCP of the ring finger.
When there is a significant deficit (3), just the MCP of the index finger is made touch by the tip of the thumb (the first finger).

Degrees of motion of the carpometacarpal joint (CMC Joint)
Measurement Position for Radial Abduction

Degrees of motion for Radial Abduction

Degrees of motion for Isolated Opposition
Calculating Loss of Use of Thumb
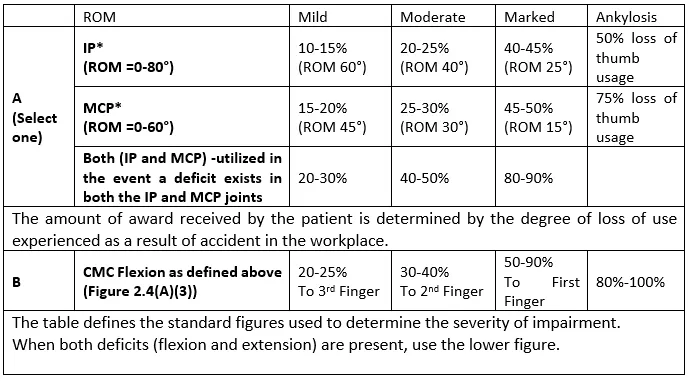
We examine whether any unusual circumstances exist before calculating the total schedule loss of thumb use. If not, we measure each joint separately and sum any deficit values (found in the table below) to determine the schedule loss of thumb function. The lower number is applicable when only one motion deficit (flexion or extension) is present. When flexion and extension are both present, the larger number is used.
Range of motion can be reduced to the sum of two major values when calculating schedule loss of use, and the overall schedule loss of use of the thumb cannot be greater than the value of ankylosis.
Thumb
Percent Loss of Use of Thumb
Instructions: To the extent there are deficits, add A+B unless a reduction
to the sum of two major values is in order.
Maximum value cannot exceed the value for ankylosis.
Schedule loss of use percentages for ranges of motion values above/below
those depicted here should be adjusted proportionally
If no other deficit exists:
- A mild impairment of thumb adduction corresponds to a 71.2 percent loss of thumb function.
- A mild impairment of thumb opposition results in a 10% loss of thumb function.
- A mild impairment of the radial abduction is equivalent to a 10% loss of thumb function.
- A higher schedule may be given for more significant impairments in adduction, opposition, or abduction.
Thumb Special Considerations
The following things should be taken into account while making the last adjustment to the fingers.
- Loss of active flexion or ankylosis at the CMC joint results in a complete loss of thumb function and is typically accompanied by a wrist deficit, in which case a hand schedule is created.
- The CMC joint is primarily the site of the thumb’s abduction and opposition, with potential deficits at the MCP and IP joints. This results in a slight, moderate, or severe reduction of the hand’s pinch and grasp strength. A hand schedule is provided for such circumstances.

Fingers

DIP Joint
Measuring Proximal Interphalangeal Joint (PIP) Position (Normal range of motion is 100 degrees)
3. Measurement Position for Metacarpophalangeal Joint (MCP) (Normal range of motion is 90 degrees)

MCP Joint
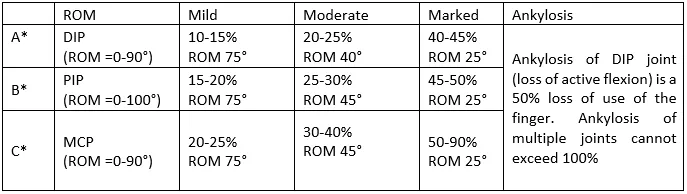
Calculating Loss of Use of Finger
First, evaluate whether any special circumstances need to be taken into account before calculating the overall schedule loss of finger use. If not, each joint should be measured separately and the values (found in the table below) summed to determine the schedule loss of use of the finger. The lower number is applicable when only one motion deficit (flexion or extension) is present. When flexion and extension are both present, the larger number is used.
For losses in all three joints, a reduction to the sum of two major values may be necessary when determining schedule loss of use, and the total schedule loss of use of the finger cannot be greater than the value of ankylosis.
Finger
Percent Loss of Use of Finger
Instructions: To the extent there are deficits, add A+B+C unless a reduction
to the sum of two major values is in order.
Maximum value cannot exceed the value for ankylosis.
Schedule loss of use percentages for ranges of motion values above/below
those depicted here should be adjusted proportionally
*Use lower figure for one deficit and higher figure when both are affected
Inquire with your doctor about your development and whether you have reached MMI. A medical report stating that you have reached MMI must be submitted to the Board by your doctor when they make that determination. The report must include an examination of the damaged bodily part and a breakdown of the percentage of functionality that has been irrevocably lost.
The report can indicate, for instance, that you function 50 percent less than you did prior to your accident. Schedule loss of use. The table shows of range of motion in different joints in the finger depending on severity and loss of use
Finger Special Considerations
Special considerations with enumerated schedule loss of use values include the following. When specified, other deficits may be introduced. However, unless special consideration number 5 below applies, the maximum schedule loss of use value cannot be greater than the value of ankylosis.
- Mallet deformity: Depending on degree, finger loss might reach 331.3 percent.
- Loss of up to 331.3 percent of the trigger finger. If the thumb or index finger is affected, choose the highest value (331.3%).
- Flail DIP joint: finger loss of 50%.
- A 50% loss of finger function results from the loss of half or more of the distal phalanx.
- Dupuytren’s contracture – Prior to schedule examination, there must be an ODNCR and/or ANCR for the condition. The accident or occupational sickness should be the only scheduled loss of use. If an impairment is identified in only one finger, there is a loss of hand function. If there are two or three, a larger schedule may be provided.
The involvement of the fingers compromises hand functionality, such as grasp strength. It is acknowledged that this may go beyond the worth of the affected finger’s ankylosis.
Loading
When multiple digits are affected, loading is the amount that is added to a schedule to account for grasp weakness or other significant loss of function. Convert multiple digit loss to an overall hand schedule when stated. Schedules with one or two digits less than 50% remain in the digits.
To calculate the overall loading value:
- To calculate the number of weeks per digit, multiply the percentage of use lost per digit by the statutory maximum number of weeks allowed per digit.
- Add the weeks for each digit together to get the “total digit weeks.”
- Multiply the “total digit weeks” by the appropriate loading percentage2, then add that amount to the “total digit weeks.”
- Divide this figure by the hand’s maximum statutory weeks (2441). To find the percentage of the hand that was lost, multiply the quotient by 100.
Example: a 50% loss of use of the index finger and a 60% loss of use of the thumb is given a 60% load and converted to a hand schedule (Scenario C below).
- (A) 50% Loss of Index 23 weeks (50% of 46 weeks)
- (B) 60% Loss of Thumb 45 weeks (60% of 75 weeks)
- Total Digit Weeks (A plus B) 68 weeks (23 + 45)
- Total Weeks including 60% load 108.8 weeks ((68 x 60%)+68)
- Converted to Hand Schedule 44.6% ((108.8/244) x 100)
Loading when two digits are affected
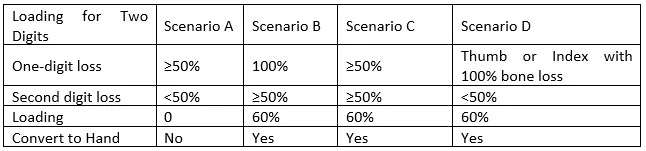
The scenarios are compared in the table when there are four different possibilities. Accidents are unplanned events, and as a result, they have varying effects on the finger depending on the type of event.
Per table above:
- Scenario A – No load is given when one digit has 50% loss of use and another has less than 50% loss of use; instead a separate percentage is given for each finger.
- Scenario B – The load is 60% and converted to a hand schedule when one digit has 100% loss of use and another digit has 50% loss of use.
- Scenario C – Schedules of 50% or more in two digits are loaded 60% and converted to a hand schedule.
- Scenario D – The load is 60% and converted to a hand schedule when there is a 100% bone loss in either the thumb or index finger and a second digit has less than 50% loss of use.
Loading when three or more digits are affected
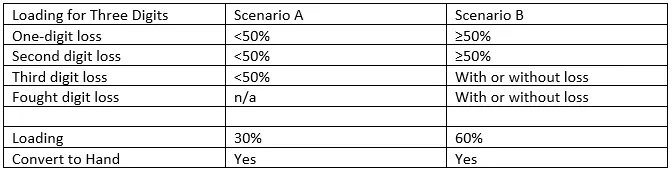
The table contrasts the circumstances where there are two separate possibilities. Accidents are unplanned events, and as a result, they have various effects according on the type of event; the finger will therefore be impacted in various ways.
Per table above:
- Scenario A – In cases of loss of three fingers with less than 50% loss of use in each finger, are given a 30% load and converted to a hand schedule.
- Scenario B – Schedules of 50% or more loss in two or more digits are loaded 60% and converted to a hand schedule.
Loading for Amputations
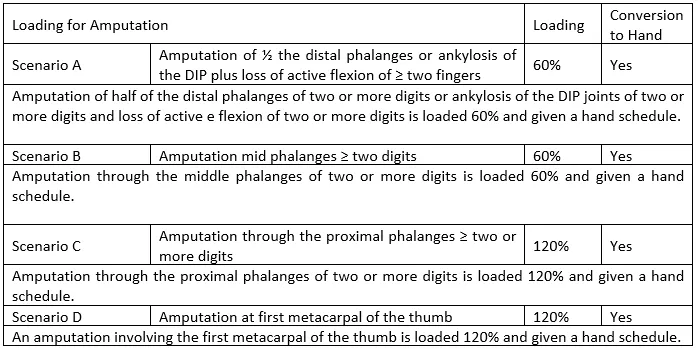
It can be incredibly devastating to have a work-related injury that necessitates the amputation of a finger or thumb. This can have severe long-term effects on the wounded person’s life. A finger amputation injury can be extremely painful, make it difficult for you to perform daily tasks, and in some cases, require the victim to change their line of work if they are unable to perform their job.
You might be entitled to file a finger amputation at work claim for compensation if an accident at work caused you to suffer a finger injury that required amputation.
Amputation
The level of amputation determines the residual disability and functional loss. It may be misleading to rely just on initial x-rays or reports. To achieve appropriate closure or improved function, the operative amputation is typically carried out at a higher level. To determine the level of bone loss and the precise level of amputation, additional post-operative x-rays are required if there is any uncertainty.
The schedule loss computation will require this information. In the worst scenarios, a finger, a portion of a finger, or multiple fingers/thumbs may need to be amputated, which would have an immediate impact on your ability to return to work since the majority of jobs require some sort of input from the hand or fingers.
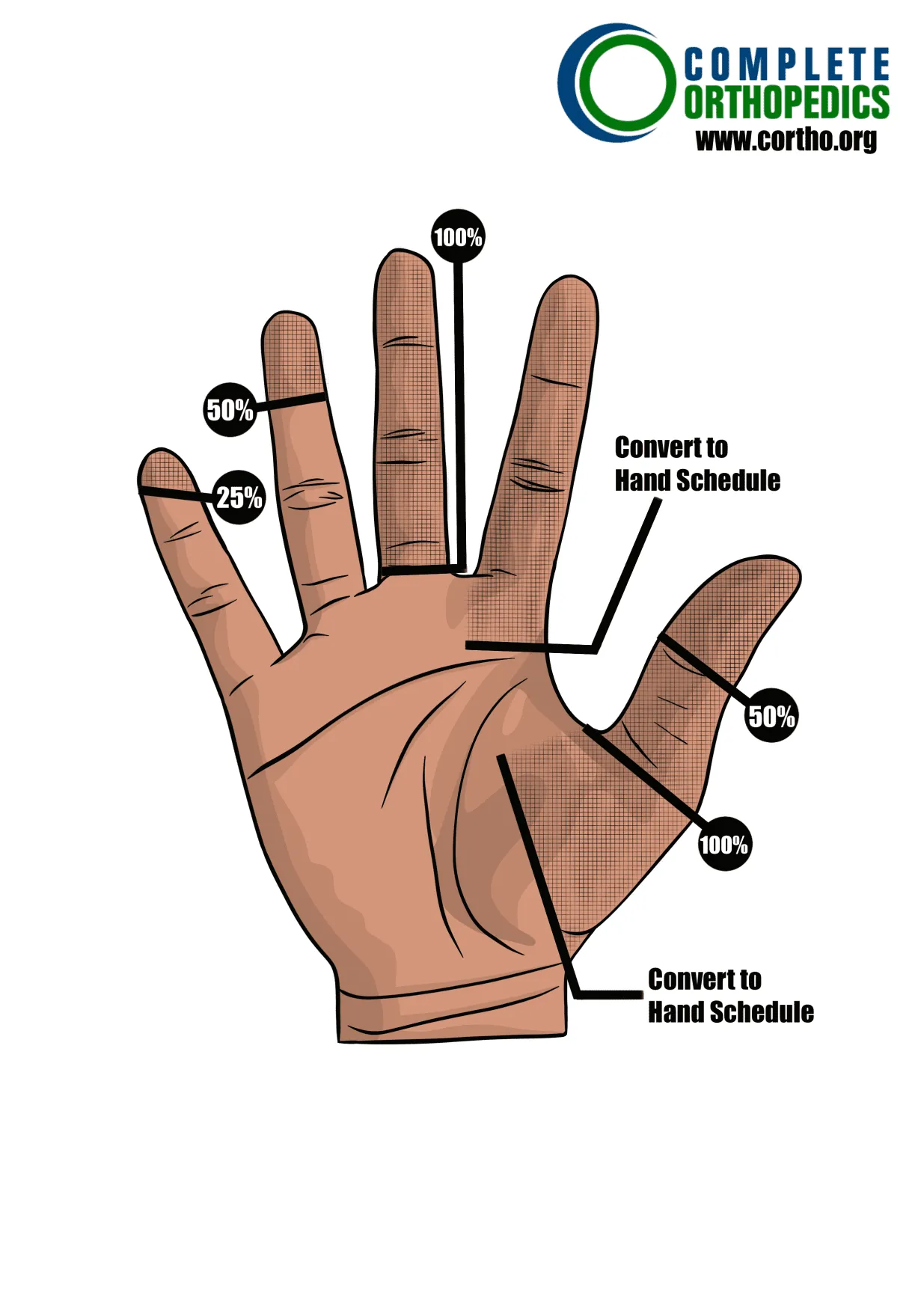
Schedule Loss of Use of the Fingers Due to an Amputation
- Complete loss of hand function results from the loss of all fingers at the proximal phalanges.
- Loss of the distal phalanx’s tuft tip (combined with bone loss) results in a 15% to 20% reduction in finger function. Add percentage for mobility deficit at the DIP joint if present.
- A loss through the base of the tuft results in a 33 ⅓% loss of finger function.
- A finger loses 50% of its function if the distal phalanx, or all of it, is lost (no additional values added for mobility impairment at the DIP joint).
- Amputation via the DIP joint results in a 50% loss of finger function.
- Complete loss of finger function results from the removal of any part of the middle phalanx.
- Any damage to the proximal phalanx results in complete loss of finger function.
- 75 weeks are equal to a thumb that is completely useless. A load of 120% and a hand regimen are used in situations of amputation close to the MCP joint.
- A loss affecting the entire finger and any portion of the ray (metacarpal) results in a 100% loss of digit function, is loaded at a rate of 120%, and is converted to a hand schedule.
- In cases where 100% was given for a member, additional schedules may be given for subsequent injuries under certain circumstances, e.g., amputation above the elbow receives 100% loss of the arm.
Please refer to the Workers Compensation Board website of your state or speak with your Workers Compensation attorney for more information.
