Look no farther if you’ve been hurt at work and are wondering about the “Scheduled Loss of Use” (SLU) on your ankle and foot. You could qualify for a compensation payment if you meet the Workers’ Compensation Board’s criteria.
If you are injured on the job, you may be eligible for a compensation payment that is determined by the Workers’ Compensation Board’s standards.
Because of your work-related accident, you have lost function in the injured body part that will last a lifetime, according on our assessment. Our evaluation follows Workers’ Compensation Standards for Assessing Ability to Work. The terms of this article are based on New York state workers compensation regulations.
Objectives for Determining Ankle and Foot Impairment
The distal tibia and fibula come together to form the ankle, a mortise joint that aids in walking by stabilizing the lower limbs. During the gait cycle, the foot serves as a sturdy platform during toe off and a shock absorber during heel strike. Ankle dorsiflexion is necessary to ascend and descend steps, whereas plantarflexion raises the body and presses pedals to operate machines or vehicles.
Our objective is to precisely determine the permanent physical limitations that a patient experienced as a result of their accident. The assessment should, to the greatest extent feasible, be based on factual information gleaned from the history and physical examination, as well as any relevant diagnostic test results.
Techniques for Determining Permanent Impairment
At the point of greatest medical improvement, when further healing is not anticipated, we evaluate the degree of permanent physical limitations. Based on the results of the clinical course of treatment, the medical provider’s experience, and any additional treatment alternatives accessible to you, the maximum medical improvement is assessed.
Where appropriate, the contralateral extremity and expected/normal values should be taken into account by the medical professional when determining the extent of permanent residual physical deficits. The interval between an injury and the point of greatest medical progress can vary, although in most situations it is one year after the injury or the most recent surgery.
When a patient develops ankylosis, needs an amputation, or loses the ability to use a certain bodily part, they incur a planned loss. Ankylosis, a disorder that causes stiffness and immobility, is caused by the body’s inflammatory reaction to the fusion of bones.
Ankle Range of Motion
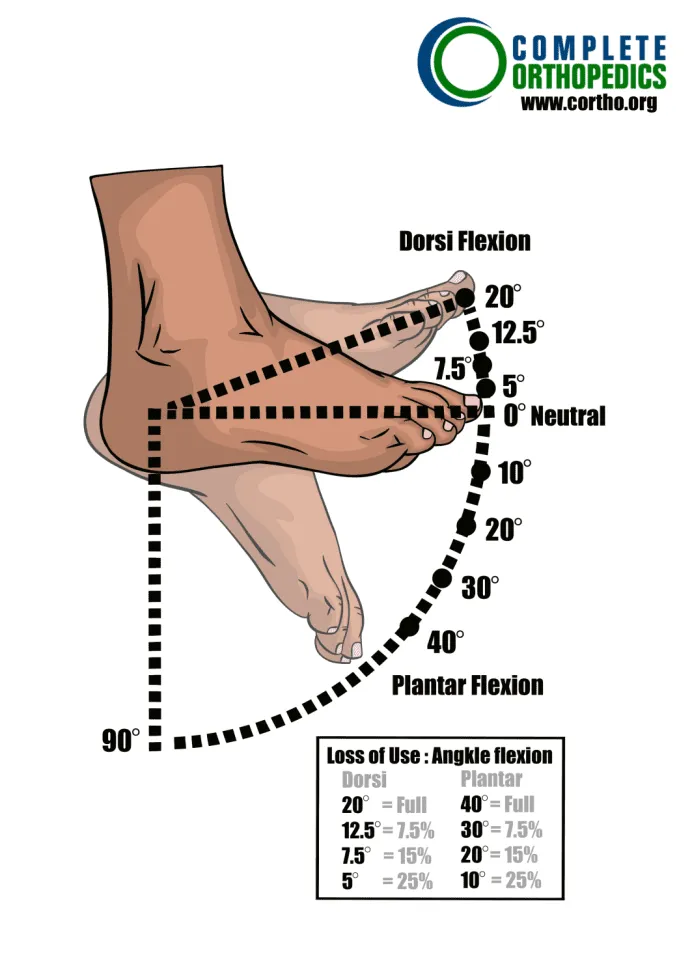
Percentage Loss of Use of the Foot: Flexion Deficits of the Ankle
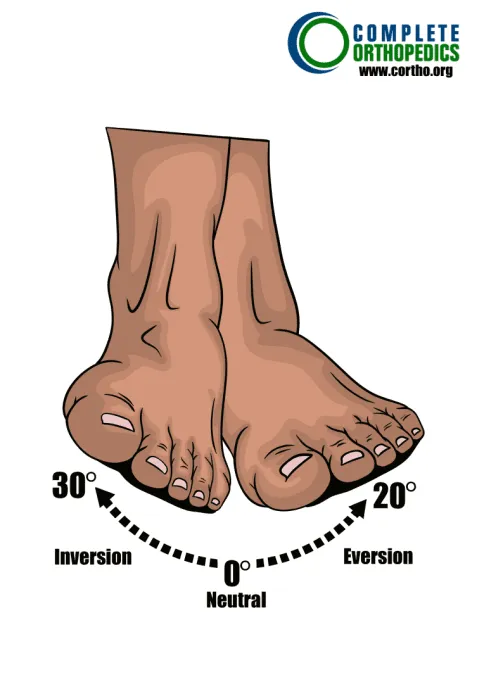
Subtalar Joint Motion
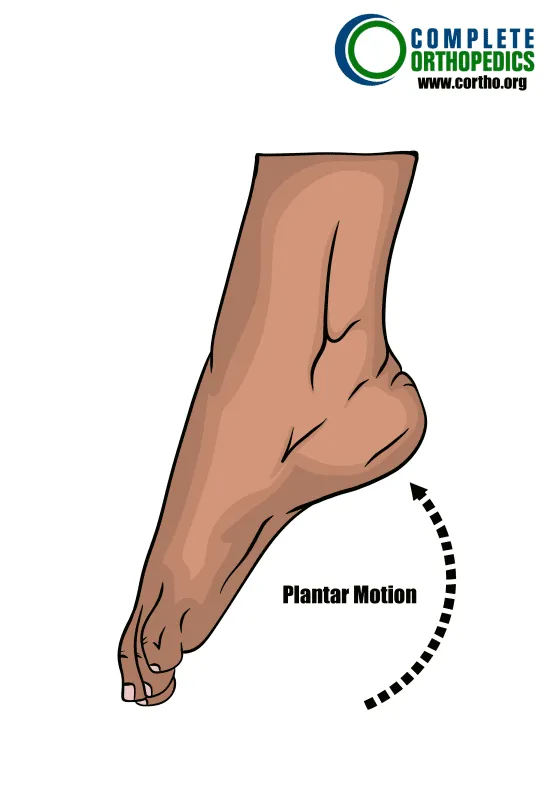
Plantar Motion
Determining Loss of Foot Use
First, we establish if any particular circumstances need to be taken into account before calculating the total schedule loss of foot use. If not, include any dorsiflexion and plantar flexion deficiencies. Other deficits, if any, may be taken into account according to the additional tables below. The value of ankylosis cannot be greater than the range of motion values.
Foot
Percent Loss of Use of Foot
Instructions: To the extent there are deficits, add A + B; other deficit values
may be considered as noted below.
Marked deficits in all cannot exceed 50-55%.
Schedule loss of use percentages for ranges of motion values above/below
those depicted here should be adjusted proportionally.

Other deficits

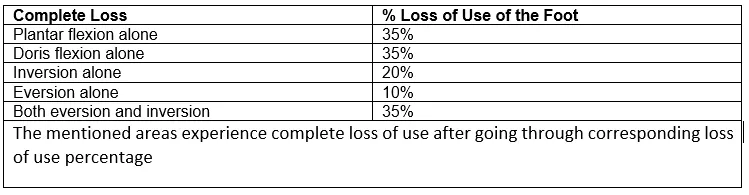
Complete Loss
Work-related foot injuries fall into two main groups. Foot injuries from lacerations, crushes, sprains, and punctures fall under the first group (cuts). Slip, trip, and fall injuries are included in the second category of injuries. Although foot injuries from slips and falls are not usually the result, neglecting foot safety plays a significant role in their occurrence.
‘
However, the breadth of foot issues at work is not limited to these two categories of foot ailments. Other ailments that affect workers frequently. Even while these might not technically qualify as occupational injuries, they can nonetheless have a significant impact on workplace health and safety.
Special considerations used by us
Special considerations with enumerated schedule loss of use values include the following. When indicated or when no schedule value is given, other deficits may be introduced. With the exception of special considerations three and four, the maximum schedule loss of use value cannot, however, be greater than the value of ankylosis.
- Schedule losses must be supported by the identification of enduring residual deficits; take into account tissue loss, mobility issues, sensory and motor impairments, and decreased function.
- Os calcis fracture results in a 33 ⅓-40% loss of foot function on average, depending on remaining mobility impairments. A leg program should be provided if the reduction of heel height shortens the leg.
- If there are other toe deficits, ankle fusion results in a loss of foot function of 75%, exceeding the 60% loss of function seen with ankylosis.
- A complete foot drop results in a 66 ⅔% loss of foot function, while a partial foot drop results in a range of 20 to
- You might want to give significant residual neurological deficits a larger schedule award.
- A ruptured Achilles tendon results in a 20–25 % of the foot on average.
- Malleolar fractures, whether bimalleolar or trimalleolar, result in a 20–30% loss of the foot on average.
Amputation
Amputation at the ankle joint results in a scheduled loss of leg function of 75%.
Amputation may be caused by serious trauma to the limb which could be crush or even blast; it could also result from severe infection to the limb. It is usually done at the last resort because it can be life altering
Please refer to the Workers Compensation Board website of your state or speak with your Workers Compensation attorney for more information.
