If you were injured at work and are curious about the “Scheduled Loss of Use” (SLU) on your knee and shin bone, look no further! If you fit the Workers’ Compensation Board’s criteria, you could receive a compensation payment.
Our report will state that because of your work-related accident, you have lost function in the injured body part, which will last a lifetime. In our report, we follow the Workers’ Compensation Guidelines for Determining Impairment.
Objectives for Determining Knee and Tibia Impairment
The knee supports the body’s weight and enables knee flexion and extension, which allow the body to be lowered to the ground and lifted, respectively. Walking is made possible by knee mobility, which also allows the body to rotate.
The objective is to precisely determine the long-term physical deficit that the patient experienced as a result of their accident. The assessment should, to the greatest extent feasible, be based on factual information gleaned from the history and physical examination, as well as any relevant diagnostic test results.
Techniques for Measuring Permanent Impairment
At the point of greatest medical improvement, when further healing is not anticipated, the degree of a permanent residual physical deficit should be assessed. Based on the results of the clinical course of treatment, the medical provider’s experience, and any additional treatment alternatives accessible to the patient, the maximum medical improvement should be assessed.
Where appropriate, the contralateral extremity and expected/normal values should be taken into account by the medical professional when determining the degree of permanent residual physical deficit. The interval between an injury and the point of greatest medical progress can vary, although in most situations it is one year after the injury or the most recent surgery.
The mechanism of the damage has very little effect on how severe the permanent residual physical deficit is. In addition to physical injury to bone, muscles, cartilage, tendons, nerves, blood vessels, and other tissues, it can also reflect the permanent residual physical deficit at the point of maximum medical improvement.
A lot of things are taken into consideration when measuring permanent impairment and as such it should be handled by experienced doctors authorized by the workers compensation board. Since the human knee is made up of numerous distinct bones, cartilages, ligaments, tendons, and muscles, there are numerous knee elements that you could hurt in a workplace accident.
Any kind of knee injury can render you incapable of moving and be excruciatingly painful. Your ability to move may be significantly impacted by even a small knee injury involving ligaments and tendons, but a serious knee injury may result in lifelong impairment.
Knee Range of Motion
Knee flexion
Flexion is measured by fully extending your knee forward while you are seated. We bring the heel of the foot as far back toward the chair as we determine the angle generated by the axis of the femur and the fibula. 0 degrees of extension to 140 degrees make up the full range of motion (complete flexion). It is represented in the table below

Knee Flexion
Knee extension
An extension deficit is the angle of loss from zero while the patient is standing with their knee completely extended. The phenomenon is expressed in the table below
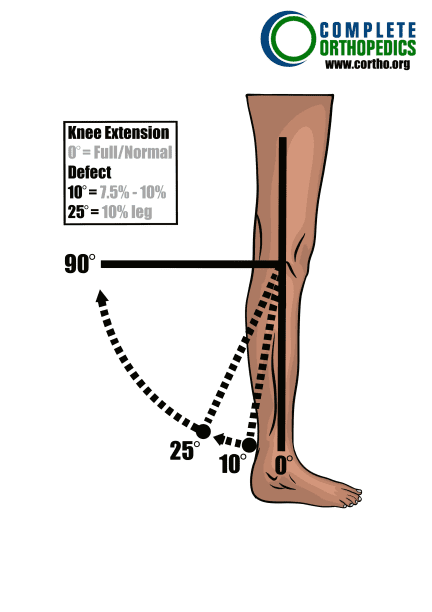
Knee Extension
Calculating loss of use
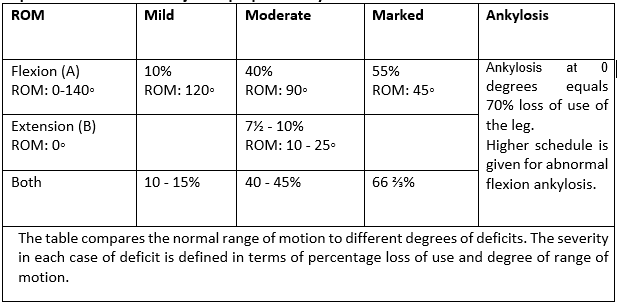
Determine whether any special circumstances need to be taken into account before calculating the overall schedule loss of knee function. If not, take into account flexion (A) or extension (B) deficits according to the chart below, as appropriate. The schedule cannot exceed the value for ankylosis when evaluating based on range of motion.
Knee
Percent Loss of Use of Knee
Instructions: To the extent there are deficits select one from the table below.
Maximum value cannot exceed the value for ankylosis (70%).
Schedule loss of use percentages for ranges of motion values above/below those
depicted here should be adjusted proportionally
7.5 Special considerations we use
Special considerations with enumerated schedule loss of use values include the following. When indicated or when no schedule value is given, other deficits may be introduced. However, the value of ankylosis cannot surpass the maximum schedule loss of use value.
- Patella: Total excision results in a 15% loss of leg function; partial excision results in a 7½–0% loss of function. Include for muscular atrophy and mobility deficits
- A patella fracture with internal fixation results in a 71/2 to 10% loss of leg function.
- Depending on the severity of the residual damage, recurrent patellar dislocation with or without surgery results in a 10-15% loss of leg function.
- Depending on the degree of mobility impairments and muscle atrophy present, chondromalacia patella, ranging from moderate to significant, results in a 7½ – 10% loss of function of the leg.
- Prepatellar or infrapatellar bursitis results in a 0 – 7½ % loss of leg function.
- A quadriceps tendon and patella ligament rupture results in a 10 to 15% loss of leg function.
- 10 – 15% of a leg’s function is lost in a tibial plateau fracture.
- Depending on the degree of residual disability, osteochondritis desiccants, with or without surgery, results in 7½ – 10% a loss of use of the leg.
- Knee instability cannot be scheduled unless it is treated surgically. If surgery is unsuccessful and there is continued instability that necessitates the use of a brace, consider categorization. Loss of use of the leg is scheduled for ligament laxity (anteroposterior or lateral medial).
- Take classification into account when an amputee’s non-functional prosthesis has lingering symptoms and problems such neuromas, phantom pain, and chronic ulcers.
- Repeated locking of the knee may not be schedule-compatible and should be classified.
- A healed tibial shaft fracture with no alignment issues results in a 0–10% loss of leg function.
- Complete or partial knee replacement or arthroplasty: The goal is to restore joint function. Results are evaluated at least a year following surgery because clinically meaningful changes in functioning can happen earlier. The schedule is determined by:
- Range of motion (ROM) as evaluated by flexion and extension (using the measurement that corresponds to the level of impairment);
- Position:
- alignment (Varus or valgus deformity),
- stability (medial/lateral [ML] laxity),
- anteroposterior (AP) motion,
- or leg length (LL)
- Atrophy (measured at mid-thigh relative to the contralateral side); and
- Presence of chronic problems (unless classification is appropriate).
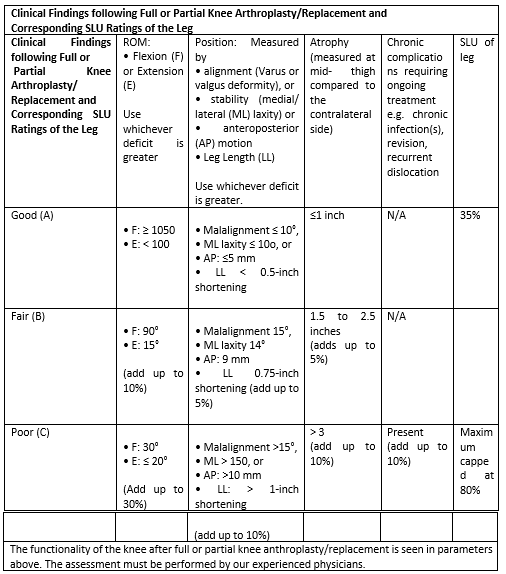
The chart below is used to calculate the schedule loss of usage values. A 35% schedule loss of use is a good result (as shown in Row A below). Add the value for the additional deficit (using the number that most closely fits the deficit in each column) to the base of 35 % to determine the total schedule loss of use award where deficits are greater than those described in Row A.
Full or Partial Knee Replacement Schedule Loss of Use
Example:
An individual undergoes surgery to replace their knee. The medical professional discovered a bad outcome with very little flexion (limited to 300) and a 150 malalignment at the point of maximum medical improvement.
- The replacement’s value would begin at 35%.
- Increase by 30% if your flexion deficit is severe (300).
- Increase by 5% for misalignment (15 degrees).
This person would have a % SLU value overall.
Amputated Leg
Amputation at the knee joint results in a 100% loss of leg function; six inches below the knee results in a 95% loss of function; and mid-calf results in a 90% loss of function. An amputee who has obtained a 100% loss of limb use may be eligible for an additional schedule award in the event of a future injury.
Amputation can really cause severe damage to the patient’s earning capacity. It can be a life distorting situation both physically and mentally. Proper assessment should be done in order to grant the patient appropriate award for schedule loss.
Please refer to the Workers Compensation Board website of your state or speak with your Workers Compensation attorney for more information.
