If you’ve been hurt at work and are wondering what “Scheduled Loss of Use” (SLU) entails for your shoulder, you’ve come to the correct spot! You could be eligible for a compensation payment determined by the Workers’ Compensation Board’s guidelines.
We will state that as a result of your work-related accident, you have lost functioning in the harmed body part and will suffer from it for the rest of your life. Our report will use Workers’ Compensation Guidelines for Determining Impairment to evaluate your case. The requirements of this article are derived from New York state workers compensation rules.
In our report we will state that as a result of your work-related accident, you have lost use of the injured body part and will be afflicted with it for the rest of your life due to your inability to work in that area. Our analysis will utilize Workers’ Compensation Guidelines for Determining Impairment to evaluate your claim. We follow the guidelines from provisions in New York state workers compensation legislation.
Objectives for Determining Impairment for Shoulder
In order to arrange the hand in space and enable functional use of the upper extremities, the shoulder and elbow are crucial. The torso and upper arms are joined by the shoulders. The shoulder joint is the most complicated and flexible joint in the human body. The shoulder is where three bones, about a dozen separate muscles, and several ligaments and tendons come together.
We can move our arms pretty much in any direction because to the way they are attached. The cost of this flexibility is that the shoulder is vulnerable to injury. Furthermore, determining the source of shoulder pain is not always simple. The capacity to complete work duties might be significantly impacted by an injury and its associated constraints.
The objective is to precisely determine the permanent physical deficit that the claimant experienced as a result of their accident. The assessment should, to the greatest extent feasible, be based on factual information obtained from the history and physical examination, as well as any relevant diagnostic test results.
Methods Available to Assess Permanent Impairment
At the point of greatest medical improvement, when further healing is not anticipated, the degree of a permanent residual physical deficit should be assessed. Based on the results of the clinical course of treatment, the medical provider’s experience, and any additional treatment alternatives accessible to the patient, the maximum medical improvement should be assessed.
The medical professional should, when appropriate, take into account expected/normal values and the contralateral extremity when assessing the level of permanent residual physical deficit. The time from the injury to the point of greatest medical improvement may differ, although in most situations it is one year since the injury or the most recent surgery.
The mechanism of the damage has no effect on how severe the permanent residual physical deficit is. In addition to physical injury to bone, muscles, cartilage, tendons, nerves, blood vessels, and other tissues, it also indicates the physical deficit that still exists after the point of maximum medical improvement.
Shoulder Range of Motion
Shoulder motions include:
- Flexion and extension
- Abduction and adduction
- External and internal rotation
Shoulder
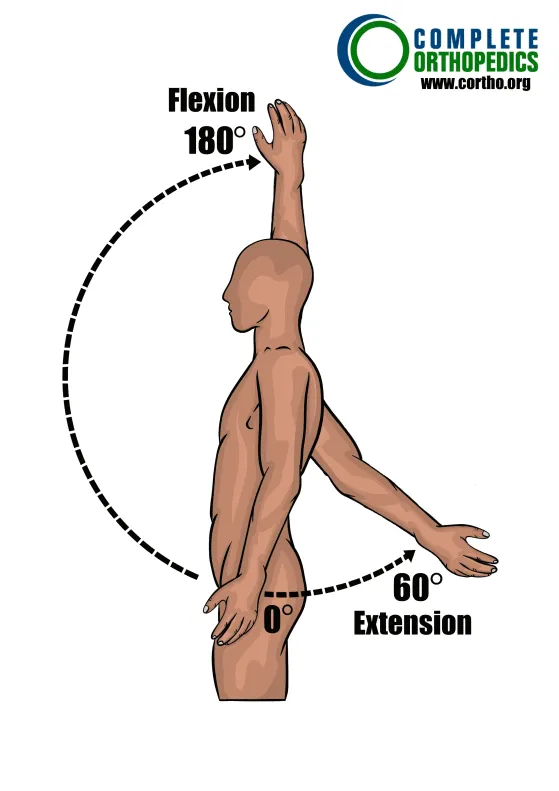
Flexion and Extension
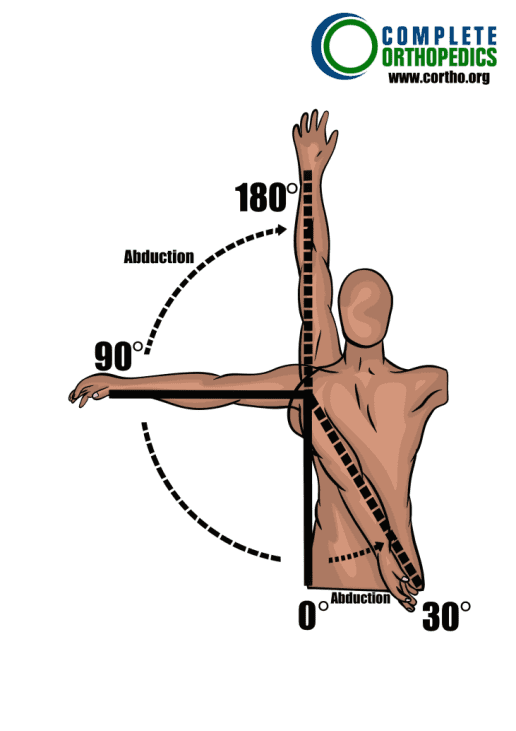
Shoulder Abduction and Adduction
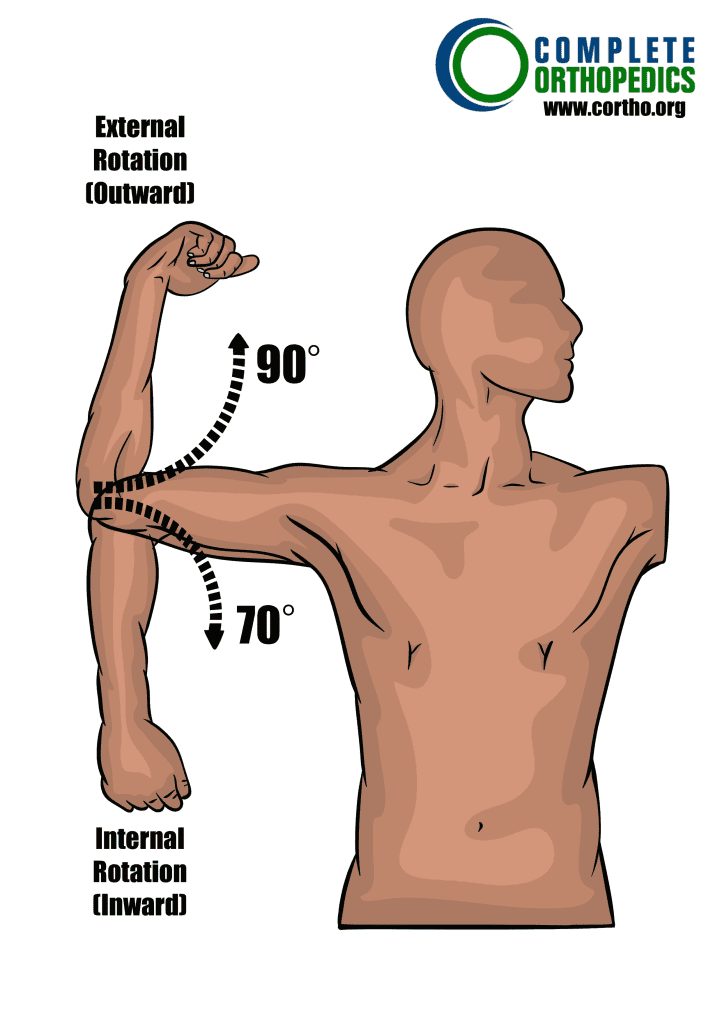
Shoulder External (Up) and Internal (Down)
Calculating Loss of Use
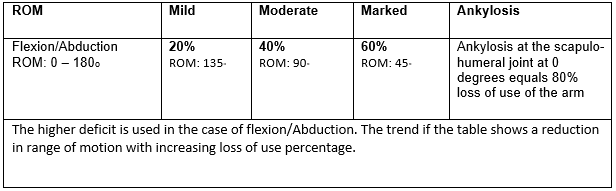
Determine whether any unusual circumstances exist before calculating the overall schedule loss of shoulder function. If not, apply the larger deficit where there are deficits in abduction and flexion (see chart below). For other considerations, see the notes. When evaluating using range of motion, the combined total deficit cannot be greater than the value of ankylosis.
Shoulder
Percent Loss of Use of Shoulder
Instructions: To the extent there are deficits select values per the chart and/or notes below.
Maximum value cannot exceed the value for ankylosis.
Schedule loss of use percentages for ranges of motion values above/below those
depicted here should be adjusted proportionally.
Note:
- The bigger of the two deficits, not both, must be used if flexion (forward elevation) and abduction deficits are both reported. However, up to 10% may be added to the overall timetable loss of use, up to and including ankylosis, if the deficit in both ranges of motion is considerable or more and the measurements are within 100 of one another.
- To avoid cumulative values, do not add slight rotational internal and exterior deficits. Add 10-15%, but not more than ankylosis, for clearly noticeable rotational impairments and muscular atrophy.
- Mild deficits of posterior extension equal 7½–10% loss of use of an arm.
- Mild deficits of adduction equal 7½ –10% loss of use of an arm.
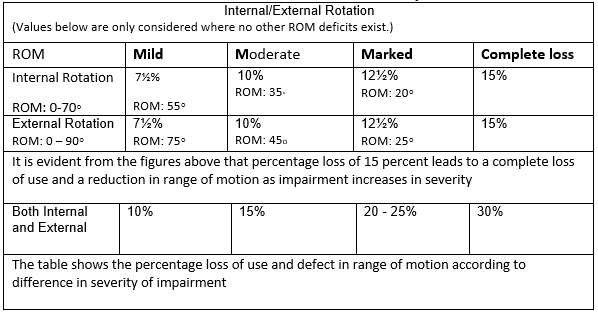
- Use the table below for isolated internal/external ROM deficiencies.
Shoulder
Internal and External Rotation Only
Special Considerations used by us
Special considerations with enumerated schedule loss of use values include the following. When indicated or when no schedule value is given, further deficits may be introduced. However, the value of ankylosis cannot surpass the maximum schedule loss of use value.
- Shoulder dislocations may be eligible for a schedule loss of use review if at least a year has passed since the corrective surgery was performed, or if the dislocation has occurred more than once and a permanent impairment has developed. An overall schedule and allocation are required in cases with pre-existing, recurrent shoulder dislocation.
- Depending on the severity of the impairment, clavicle fractures might range from 0 to 10 %.
- Loss of arm function from acromio-clavicular or sterno-clavicular separation ranges from 7½ to 10 percent.
- Depending on the severity of the functional impairment, a winged scapula caused by Serratus Anterior Palsy and/or Trapezius Palsy may result in a 15-20% loss of arm function. In these situations, wait two years after a main nerve has been surgically repaired before evaluating for a schedule loss.
- Bone loss from resection of either end of the clavicle is equal to 10%; loss of arm function after resection of the entire clavicle is equal to 15%. If present, take into account the most prominent mobility deficits in connection to functional deficit.
- A non-surgical rupture of the biceps muscle’s long head results in a 10 to 15 percent loss of arm function. A biceps tear at the distal point of insertion results in a 20% reduction in arm strength. The timeline may vary by up to 33 ⅓% loss of arm function, taking into account muscular weakness and mobility, depending on the severity of the impairment discovered.
- Frozen shoulder and adhesive capsulitis (with or without surgery): Provide a plan for loss of function if the problem is asymptomatic.
- The supplied schedule is concentrated on the extremity’s most valuable portion. Calculate the main loss in the part affected first in the event of a high schedule for one specific part of the extremities. For instance, amputation at the wrist results in a 100% loss of hand function or an 80% loss of arm function. The end timetable would be 90 percent loss of use of the arm if there were subsequent deficits of the elbow and/or shoulder, which would be added to the initial 80 percent loss of use of the arm by 10%.
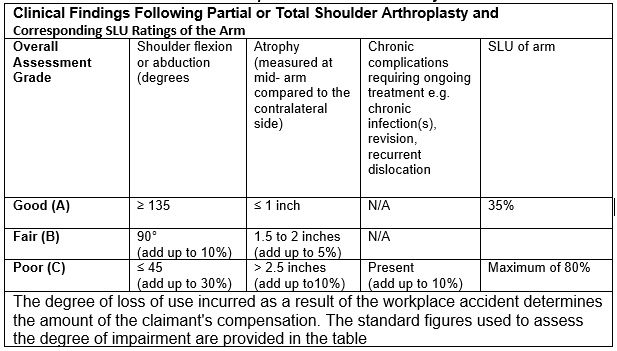
- Results of full or partial shoulder arthroplasty or replacement are evaluated no earlier than 12 months following surgery because clinically meaningful changes in functions can take place earlier. The schedule is provided in accordance with the medical evaluation of:
- range of motion as measured by flexion or abduction, utilizing the most severe degree of impairment;
- atrophy as measured at the mid-arm level and compared to the contralateral side; and
- the presence of chronic problems as shown in the table below (unless appropriate for classification).
The chart below is used to calculate the schedule loss of usage values. A 35 % Schedule Loss of Use is considered to be a positive result (as shown in Row A below). Add the value for the additional deficit (using the value that most closely matches the deficit in each column) to the base of 35 percent to determine the total schedule loss of use award where deficits are greater than those described in Row A.
Shoulder Joint Replacement Schedule Loss of Use
Example
An individual undergoes surgery to replace their shoulder. The medical professional discovered a satisfactory outcome with full range of motion but some atrophy present at the point of optimum medical progress. Starting with the initial value for a positive outcome (35%) and adding % for the atrophy if the atrophy measurement was:
- 1.5 inches less than the contralateral side (overall SLU value for this individual would be 40%)
- If the distance is more than 2.5 inches from the other side, increase it by 10%. (overall SLU of 45 percent).
Amputation
Amputation from the elbow to the shoulder results in a complete loss of arm function. Amputation can seriously harm a claimant’s ability to earn money. It has the potential to physically and mentally alter their life. For the claimant to receive the proper award for schedule loss, a proper evaluation must be made. Since it is essentially the worst-case scenario, it is always a last resort.
Please refer to the Workers Compensation Board website of your state or speak with your Workers Compensation attorney for more information.
