If you were injured while on the job and are questioning what effect “Scheduled Loss of Use” (SLU) means for your hip, look no further!
You could be eligible for a compensation payment that is determined by the Workers’ Compensation Board’s regulations.
Our SLU report will conclude that you have permanently lost function in the injured body part due to your work-related accident. The determination of impairment is based on New York state workers compensation guidelines.
Walking, climbing stairs, and sprinting are all daily tasks made possible by the hip joint and its support structures. Where the femur and pelvis meet is where the hip, a ball and socket joint, is placed. The ball and socket design offer the hip the second-largest range of motion after the shoulder.
The goal is to precisely determine the long-term physical deficits that a patient experienced as a result of their accident. Our assessment is based on factual information obtained from the history and physical examination, as well as any relevant diagnostic test results.
Techniques for Measuring Permanent Impairment
At the point of greatest medical improvement, when further healing is not anticipated, the degree of a permanent residual physical deficit should be assessed. Based on the results of the clinical course of treatment, the medical provider’s experience, and any additional treatment alternatives accessible to the patient, the maximum medical improvement should be assessed.
The mechanism of the damage has almost no effect on how severe the permanent residual physical deficit is. In addition to physical injury to bone, muscles, cartilage, tendons, nerves, blood vessels, and other tissues, it can also reflect the permanent residual physical deficit at the point of maximum medical improvement.
We evaluate the contralateral extremity and expected/normal values when determining the degree of persistent residual physical deficiency, if applicable. Although the time between a wound and the moment of greatest medical advancement can differ, it is typically one year following the wound or the most recent surgery.
Range of Motion in the Hip
Motions includes:
- Abduction – Coronal plane range of motion rotating about an imaginary line of an axis passing through the head of the femur. Through 45 degrees is the typical range of motion. (The lower extremity pivots away from the centre.)

- Adduction: A range of motion in the coronal plane that revolves around an imaginary axis that passes through the femoral head. A 35-degree range of motion is considered normal. Moving across the midline is the lower extremity.

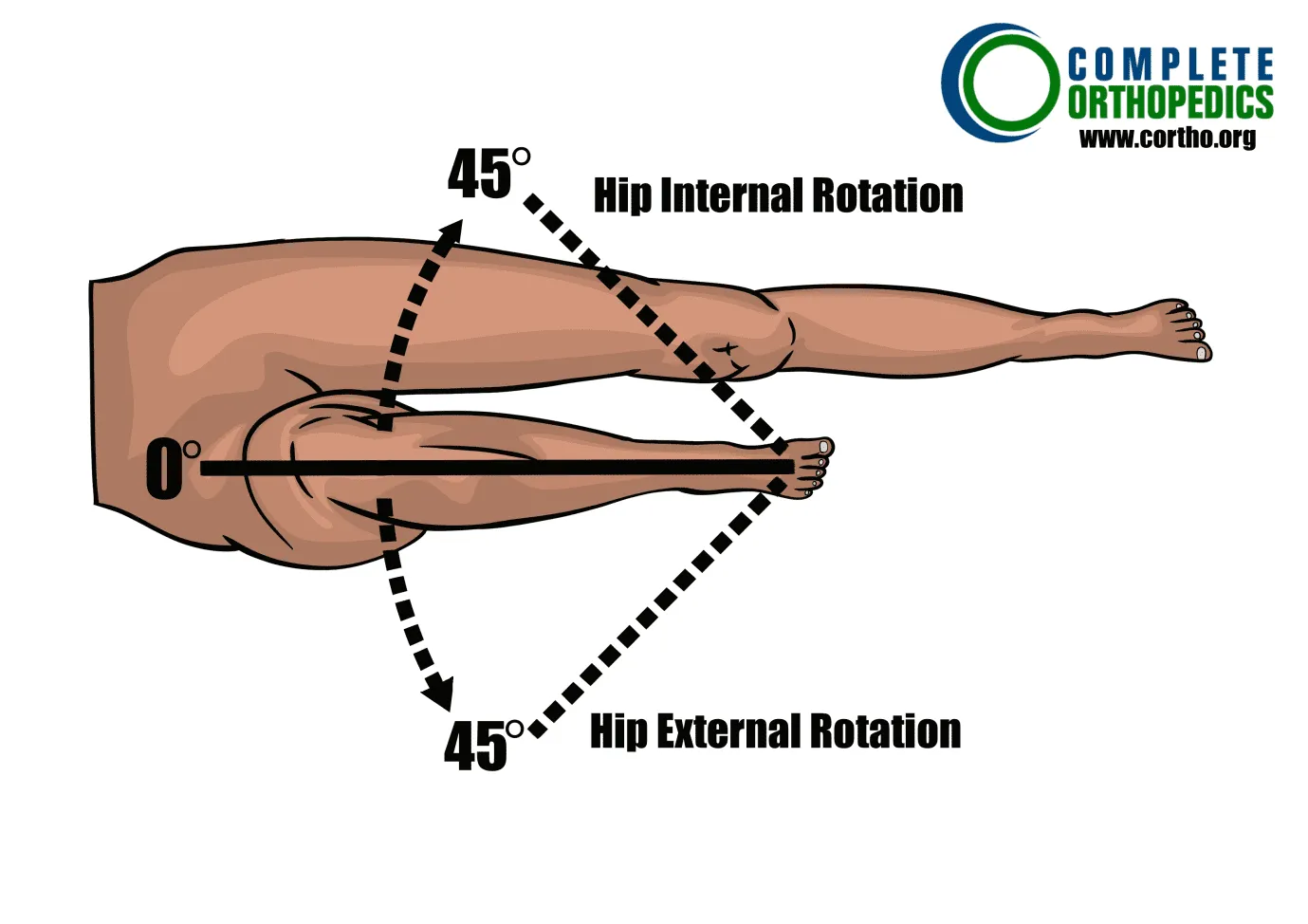
- Internal Rotation – With the foot firmly planted on the examination table, the lower extremity is partially flexed. The knee crosses across the opposing extremity as a result of the hip rotating. A 45-degree range of motion is considered normal.
- External Rotation – With the foot firmly planted on the examination table, the lower extremity is partially flexed. The knee is moved away from the opposing extremity by rotating the hip. A 45-degree range of motion is considered normal.
- Flexion (forward elevation) – Range of motion with the flexed knee moving in front of and above the waist while rotating about an axis of an imaginary line through the acetabulum in the sagittal plane. A 120-degree range of motion is considered normal

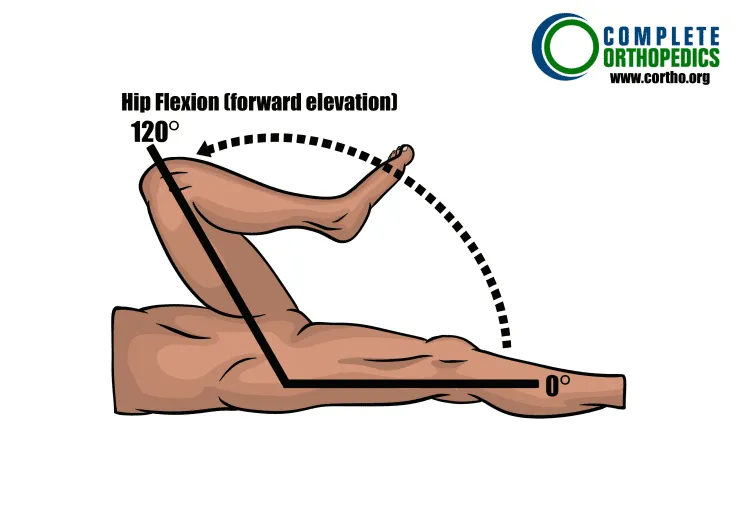
Hip Flexion
6. Extension – A 30-degree range of motion in the sagittal plane with the leg travelling behind the body on an imaginary axis through the acetabulum. Lower extremity is raised off the examination table while the patient is lying on their back.
Determining Loss of Use
First, evaluate whether any special circumstances need to be taken into account before calculating the total timetable loss of hip use. If not, add abduction/adduction (A) + internal/external rotation (B) + flexion (C), to the extent there are deficits in these ranges of motion, to calculate the overall schedule loss of hip usage. As noted below, other deficits may be taken into account. The schedule cannot exceed the value for ankylosis when evaluating based on range of motion.
Hip
Percent Loss of Use of Hip
Instructions: To the extent there are deficits add A+B+C; for other deficit values see notes.
Maximum value cannot exceed the value for ankylosis.
Schedule loss of use percentages for ranges of motion values above/below
those depicted here should be adjusted proportionally.
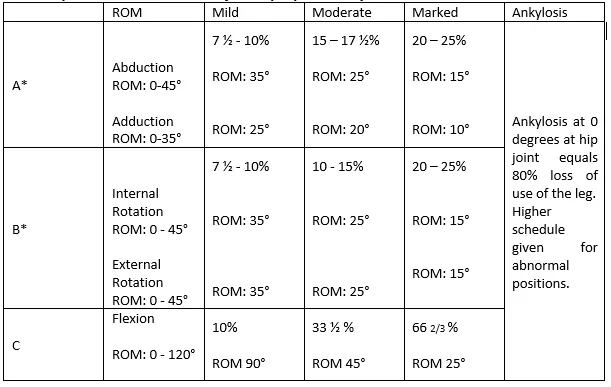
*Use lower figure for one deficit and higher figure when both are affected
A doctor usually determines the percentage loss of use of affected body part which in this case is the hip. The table above shows the comparison of the severity of injury based on percentage loss of use. A well experienced physician must carry out the medical examination to ensure that the appropriate award for schedule loss of use is given
Notes:
- Adduction and abduction: Total loss of both implies a 33½ loss of leg function
- Internal and external rotation: Total loss of both implies a 30% loss in leg function.
- A deficit in posterior extension implies in a7½ –10% loss of leg function.
Special Considerations we use for evaluation of SLU
Special considerations with enumerated schedule loss of use values include the following. When indicated or when no schedule value is given, other deficits may be introduced. However, the value of ankylosis cannot surpass the maximum schedule loss of use value.
- Femur head and neck removal without prosthetic replacement results in 50% anatomical loss of leg function. Include any mobility issues.
- An MRI revealed synovitis of the hip and bursitis in the trochanteric, ischiogluteal, and iliopsoas bursas; the schedule reward is a loss of leg function of 0-7½%. Date of assessment two or more years after the injury date
- If there is a residual hip impairment, such as limited hip joint movement and thigh muscle atrophy, a fractured pelvis may be eligible for a schedule award at the end of two years. Scheduled leg usage loss could range from 15 to 20 %.
- Leg lengthening or shortening causes a loss of use of the leg of 5% for a half-inch, for a third-inch, and 10% for a full-inch.
- In the event of a quadriceps rupture, account for 15 to 20% of deformity and weakness. Include any mobility issues. An average schedule results in a 20 to 25 % of leg function. A higher schedule should be taken into consideration if the knee is lax.
- A 10% reduction in leg function results from quadriceps atrophy and weak knee extension.
- An additional schedule award may be given to an amputee who has completely lost use of a leg following a second accident or injury as a result (e.g., hip fracture).
- Two years must pass after a hip fracture, with or without surgery, before the schedule award is finally evaluated. Request a recent X-ray of the femoral head to evaluate the bone stock and check for hardware displacement, loosening, and misalignment. If metallic hardware is removed, schedule evaluation must occur at least six months following removal and no earlier than two years after the date the hardware was installed.
- Restoring joint function is the goal of whole or partial osteotomies, hip replacements, or both. Results are evaluated at least twelve months following surgery since functional changes that are clinically important can happen earlier.
The schedule is provided based on a medical evaluation of
- hip flexion range of motion,
- leg position (including leg length discrepancy [measured, in the supine position, from the umbilicus to the tip of the distal medial malleoli] and/or mal-rotation),
- atrophy (measured at the mid-thigh as a comparison for the contralateral side),
- and the presence of chronic complications, as shown in the table below (unless appropriate for classification).
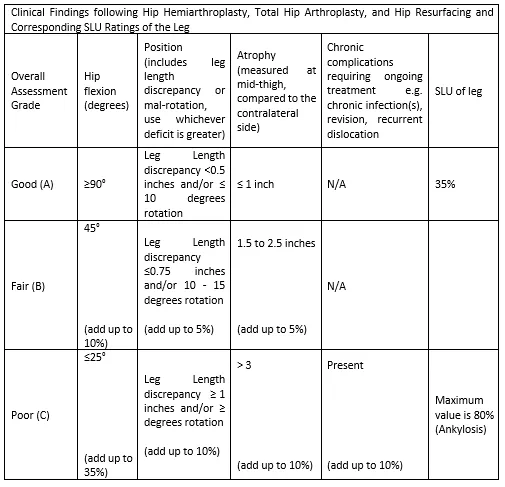
The chart below is used to calculate the schedule loss of usage values. A % schedule loss of use is a good result (as shown in Row A below). Add the value for the additional deficit (using the number that most closely fits the deficit in each column) to the base of 35 % to determine the total schedule loss of usage award where deficits are greater than those described in Row A.
Full or Partial Hip Replacement Schedule Loss of Use
Example:
A patient undergoes hip replacement surgery. The medical professional concluded that a fair outcome existed at the point of maximum medical improvement
The individual has a 20-degree mal-rotation, a .8-inch leg length difference, and a more constrained range of motion in flexion (ROM to 45 degrees).
- The replacement’s value would begin at 35%.
- Increase by 10% for a greater flexion deficit (45 degrees).
- Increase by 10% for the incorrect rotation (20 degrees).
- This person would have a % SLU value overall.
Amputation
Amputation at any point, from the knee joint to the hip joint, results in a complete loss of limb function.
Please refer to the Workers Compensation Board website of your state or speak with your Workers Compensation attorney for more information.
