If you’ve been injured at work and are wondering what “Scheduled Loss of Use” (SLU) means for your elbow, you’ve come to the correct website! You may be eligible for a compensation payment determined by the Workers’ Compensation Board’s rules. We will state that as a result of your work-related accident, you have lost functioning in the harmed body part and will suffer from it for the rest of your life.
Our report will use Workers’ Compensation Guidelines for Determining Impairment to evaluate your case. The requirements of this article are derived from New York state workers compensation rules.
Injury to the elbow can have serious effects on a person’s livelihood. An individual hurt on the job may never be able to work again, depending on the severity of the injury. When this injury occurs, the employee is entitled to submit a workers’ compensation claim for payments related to permanent total disability. Amputation injuries are one amongst many types of injuries that could prevent a worker from being able to return to work.
We’ll explain how we evaluate your SLU status for your elbow.
Objectives for Determining Impairment for Elbow
To place the hand and wrist in a way that allows for functional use of the upper extremities, the elbow is crucial. The elbow joint’s primary job is to place the hand, either by extending it outward (elbow extension), bringing it inward (elbow flexion), or moving it in a more precise way (supination/pronation).
Accurately determining the physical deficit that you sustained as a result of their disability is the objective. As much as is practical, the assessment should be based on factual findings discovered during the history and physical examination, as well as the findings of any necessary diagnostic tests.
Methods Available to Assess Permanent Impairment
At the point of greatest medical improvement, when further healing is not anticipated, the degree of a permanent residual physical deficit is evaluated. Based on the results of the clinical course of treatment, the medical provider’s experience, and any additional treatment alternatives accessible to you, the maximum medical improvement should be assessed.
Where appropriate, the contralateral extremity and expected/normal values should be taken into account by us when determining the degree of permanent residual physical deficit. The time from the injury to the point of greatest medical improvement may differ, although in most situations it is one year since the injury or the most recent surgery.
The mechanism of the damage has little effect on how severe the permanent residual physical deficit is. The physical impairment of bone, muscles, cartilage, tendons, nerves, blood vessels and other tissues is one type of permanent residual physical deficit that is reflected at the time of maximum medical improvement.
Elbow Range of Motion
Normal Range of Motion 0-150°
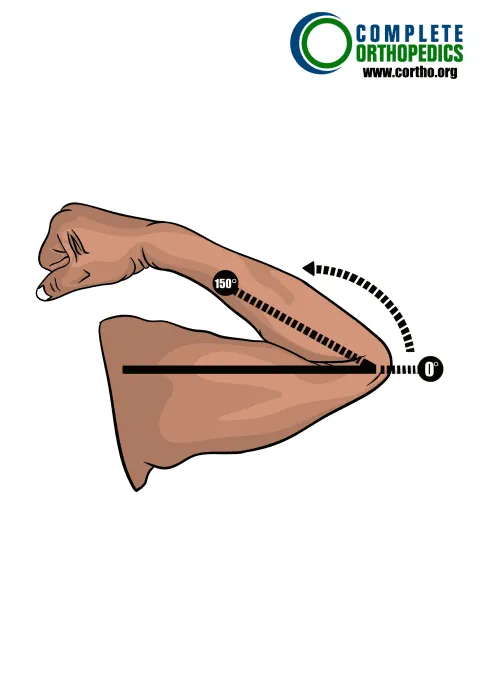
(a) Elbow Flexion
Calculating Loss of Use
We check whether any special circumstances need to be taken into account before calculating the total schedule loss of elbow function. In the absence of this, the combined deficits in extension and flexion are used to assess the overall loss of elbow function. The maximum loss of elbow function cannot be more than ankylosis when evaluating based on a range of motion.
Elbow
Percent Loss of Use of Elbow
Instructions: To the extent there are deficits, add A+B.
The maximum value cannot exceed the value for ankylosis.
Schedule loss of use percentages for ranges of motion values above/below those
depicted here should be adjusted proportionally.
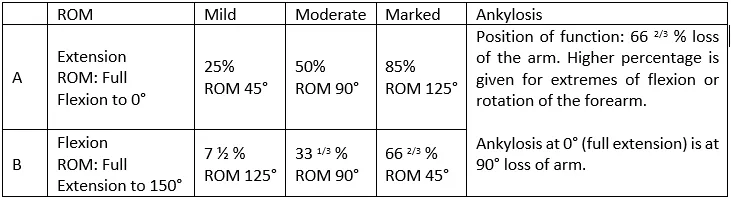
The table above compares the range of motion and percentage loss of use across the different degrees of severity
A schedule loss of use is normally calculated approximately a year after the accident or surgery date. You must first receive a diagnosis of Maximum Medical Improvement prior to doing a scheduled loss of use.
We will offer a loss of use opinion and send it to the workers compensation board. The Insurance Carrier now has the option of accepting our recommendation or seeking the advice of an Independent Medical Examiner. The opinions of the two doctors frequently differ from one another. The legislation encourages negotiation between the two perspectives, but if an agreement cannot be reached, the two doctors’ evidence is taken, and the judge will decide which doctor they feel to be credible.
Special Considerations
Special considerations with enumerated schedule loss of use values include the following. When indicated or when no schedule value is given, other deficits may be added. However, the value of ankylosis cannot surpass the maximum schedule loss of use value.
- When mobility issues are taken into account, a loss of the radius head results in a 10% reduction in arm utilization.
- Loss of arm function due to elbow laxity and hyperextension deficiency is between 10 and 15 percent.
- Medial and lateral epicondylitis often receives a schedule, but if it develops into a chronic, severe, and incapacitating condition, the classification may be warranted.
- Osteochondral fracture and bursitis of the olecranon. Schedules are dependent on residual deficits.
- Due to bone loss and mobility deficits, olecranon excision results in a 10% loss of arm function.
Amputation
Percent Loss of Use of the Arm: Amputation at Different Levels

The table above shows the percentage loss of use of arm after amputation at different levels to give a better understanding of the consequences of the situation.
One of the most devastating and permanently incapacitating sorts of job injuries is amputation. Amputation has terrible ramifications that extend beyond only the bodily, including emotional anguish and psychological distress. Reduced mechanical stability and practical restrictions, such as increased usage of the opposing limb, can result from the amputation site.
The “phantom limb” syndrome, in which the injured claimant claims they can genuinely feel a body part that is no longer there, is another potential complication following amputation. Phantom pain can cause aching, burning, and even movement as symptoms.
According to researchers, these symptoms are related to how the brain and body interact, which causes the rest of the brain to receive information about a limb whether it is present or not.
Please refer to the Workers Compensation Board website of your state or speak with your Workers Compensation attorney for more information.
