If you were hurt at work and are wondering what “Scheduled Loss of Use” (SLU) means for your hand and wrist, you’ve come to the correct spot! You could be eligible for a compensation payment that is determined by the Workers’ Compensation Board’s guidelines. Our report will state that because of your work-related accident, you have lost function in the harmed body part that will last a lifetime.
Workers’ Compensation Guidelines for Determining Impairment are followed in our report. The provisions of this article are based on New York state workers compensation guidelines.
We’ll explain how we evaluate your SLU status for your your hand and wrist.
Objectives for Determining Impairment for Hand and Wrist
A crucial component of the finger and thumb movements is the hand and wrist. The wrist also functions as a link between the forearm and hand’s related structures. Complex flexion/extension and radial/ulnar movements of the hand are made possible by the wrist.
Assessing the patient’s permanent residual physical deficits as a result of their injury is the objective of doing the scheduled loss of use. The evaluation should, to the greatest extent feasible, be based on facts discovered during the history and physical examination, as well as any results of necessary diagnostic testing.
Methods we use to Assess Permanent Impairment
At the point of greatest medical improvement, when further healing is not anticipated, the degree of a permanent residual physical deficit is evaluated. Based on the results of the clinical course of treatment, our experience, and any additional treatment alternatives accessible to the patient, the maximum medical improvement is assessed.
Where appropriate, the contralateral extremity and expected/normal values is taken into account by us when determining the degree of persistent residual physical deficit. The interval between an injury and the point of greatest medical progress can vary, although in most situations it is one year after the injury or the most recent surgery.
The mechanism of the injury has little impact on how severe the permanent residual physical deficit is. In addition to physical injury to bone, muscles, cartilage, tendons, nerves, blood vessels, and other tissues, it can also reflect the permanent residual physical deficit at the time of the maximum medical improvement.
Our evaluation of permanent impairment report is truthful, thorough, and impartial. We look at maximum medical improvement; the level of permanent impairment brought on by the accident or condition; and, if appropriate, the percentage of permanent impairment attributable to any prior injuries, pre-existing conditions, or abnormalities.
Our report includes accurate information based on all medical data and investigation findings, as well as the physician’s own clinical examination and history gathering. Our report will also properly cite any further reports or investigations that were used to form an diagnosis (if not already achieved a this stage).
Wrist Range of Motion
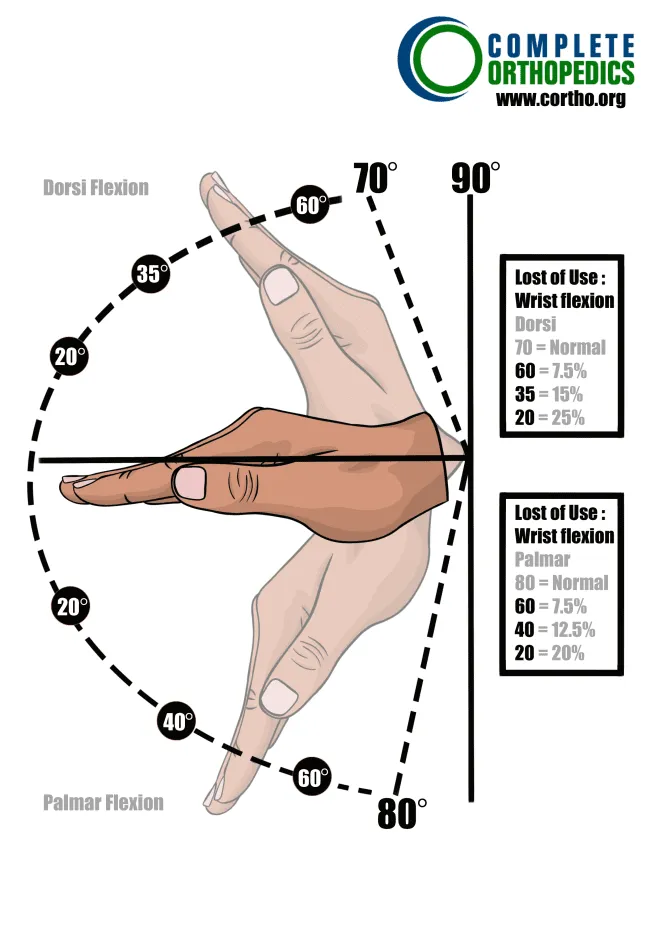
(a) Dorsi flexion and Palmar flexion of the Wrist (Percent Loss of Use of the Hand)
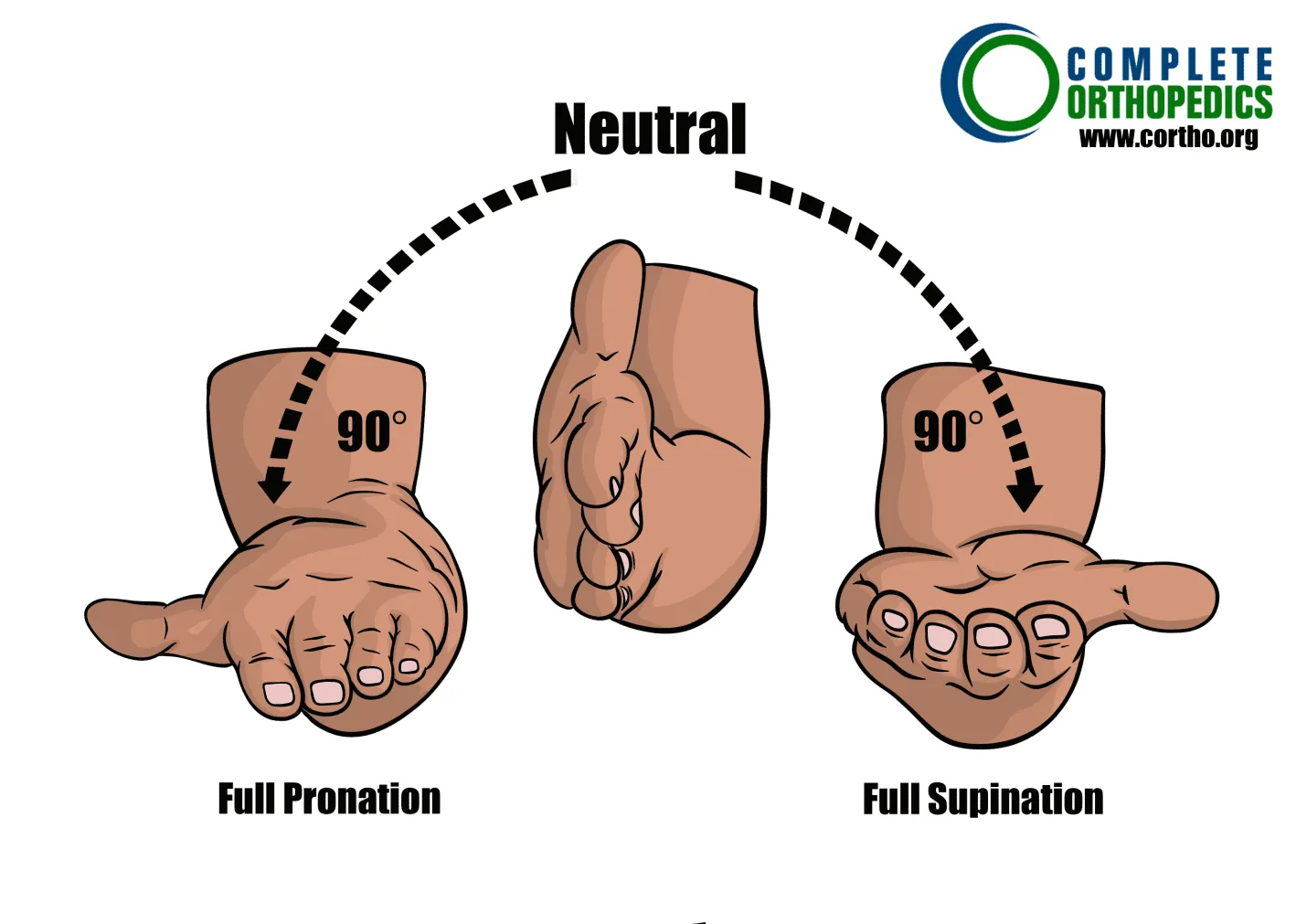
(b) Pronation – Supination of the Wrist (as measured with the elbow flexed to 90 degrees, and arm adducted along the chest wall).
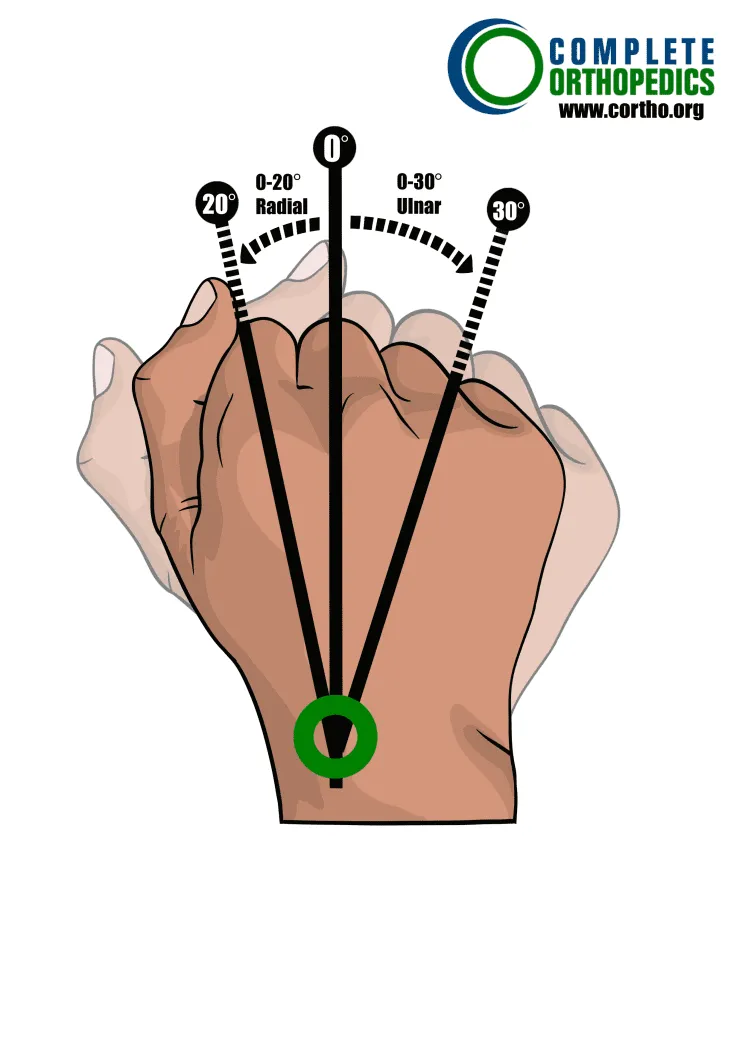
(c) Lateral Wrist Motion
Calculating Loss of Use
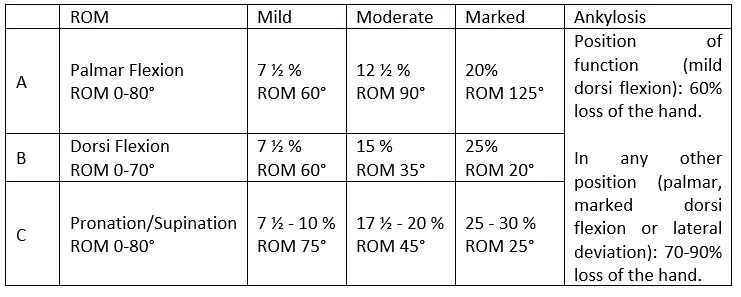
We determine whether any unusual circumstances exist before calculating the wrist’s overall schedule loss of function. If not, we add Palmar Flexion (A) + Dorsi Flexion (B) + Pronation/Supination (C), to the degree there is a deficit in these ranges of motion, to determine the total schedule loss of wrist usage. However, schedule loss of use cannot surpass 55% when there are clear limitations in all wrist motions.
Wrist
Percent Loss of Use of Wrist
Instructions: To the extent there are deficits, add A+B+C or values as indicated per notes.
Maximum value for marked cannot exceed 55%.
Schedule loss of use percentages for ranges of motion values above/below those
depicted here should be adjusted proportionally
We use a lower figure for one deficit and higher figure when both are affected
There is a monetary compensation that compensates you for the reduction in your ability to make a living due to a permanent functional impairment of the wrist brought on by your workplace injury. You loses some of their ability to earn a living depending on the part of the wrist afflicted and the type of permanent disability. The table above compares the alteration in normal range of motion based on severity of physical deficits
Additionally,
- Complete loss of Palmar flexion equals 25% loss of the hand.
- Complete loss of Dorsi flexion equals 33⅓ % loss of the hand.
- Complete loss of both pronation and supination equals 35% loss of use of the hand.
- Deficits in radial-lateral motion and ulnar motion may be separately considered if other findings in the wrist are normal.
We use the following Special Considerations
We also consider specific factors for schedule loss of use figures. If a deficit is indicated or if a schedule value is not provided, additional deficits may be introduced. Except for Special Consideration Number One listed below, the Maximum Schedule Loss of Use Value cannot, exceed the Value of Ankylosis.
- Complete wrist drop, also known as radial nerve palsy, results in a 66 ⅔% loss of hand function; partial wrist drop results in a lower percentage.
- The Darrach procedure (resection of the distal ulna) results in a 10% reduction in hand function due to bone loss and mobility issues.
- Resection of the “proximal row” carpal bones results in a 20% reduction in hand function due to bone loss alone, plus any mobility issues that may be present.
- Navicular fracture – Hold non-union cases for two years. If the X-rays show signs of clinical union (fibrous) and the pain is not severe, schedule loss of hand function. Consider classification when dealing with unusually painful situations.
- Hold until X-rays reveal a static situation if you have Kienböck’s disease (aseptic necrosis of the carpal lunate). If the problem is symptomatic, consider classification.
- Carpal Tunnel Syndrome: If asymptomatic, schedule one-year post decompression. Consider classification if symptoms persist and grow severe and incapacitating. [Values are listed in Nerve Section 10] .3A]
- Depending on the limitations, De Quervain’s disease causes a 7½-20% loss of thumb function with or without surgical release. Give a schedule for loss of hand usage if the wrist has a residual deficit and the hand’s grip strength is compromised.
- Depending on the medical findings, the wrist ganglion might range from 0- 7½%percent of the hand.
Amputation
One of the most severe sorts of workplace injuries, amputation has long-lasting effects on a worker’s livelihood and well-being. Where an injury has prevented the body from healing injured bone or tissue, surgical amputation may be required.
It becomes necessary to amputate a damaged limb when it can no longer get blood that carries oxygen and nutrients because the cells begin to slowly degenerate and lose function.
Amputation is always the last option for medical professionals due to the trauma it causes to the body and a claimant’s mental health. An amputee may require months of therapy following surgery and develop post-traumatic stress disorder.
It could imply being unable to make a living after the accident or making less money. The patients quality of life will be forever impacted by any type of amputation.
A wrist amputation results in complete loss of hand function (80 percent loss of use of the arm).
Please refer to the Workers Compensation Board website of your state or speak with your Workers Compensation attorney for more information.
