The New York State workers compensation board has developed these guidelines to help physicians, podiatrists, and other healthcare professionals provide appropriate treatment for Rotator Cuff Tears.
These Workers Compensation Board guidelines are intended to assist healthcare professionals in making decisions regarding the appropriate level of care for their patients with ankle and foot disorders. The guidelines are not a substitute for clinical judgement or professional experience. The ultimate decision regarding care must be made by the patient in consultation with his or her healthcare provider.
Rotator Cuff Tears of Shoulder Injury
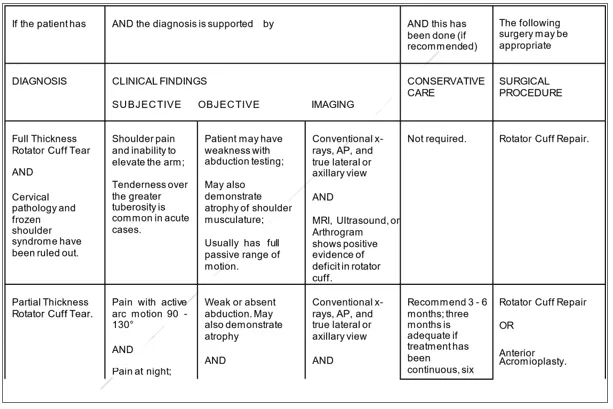
Full-thickness or partial tears of the supraspinatus tendon, which makes up the majority of rotator cuff injuries, can result from vascular, traumatic, degenerative, or a combination of these reasons. A big tear is greater than five centimetres, typically with retraction, and smaller tears are those that are less than one centimetre, one to three centimetres, three to five centimetres, and less than one centimetre.
History and Mechanism of Injury of Rotator Cuff Tears
- Mechanism of Injury: based on repetitive overhead motions with internal or external rotation or acute overuse injuries to the shoulder.
- History could include of
- Most partial-thickness cuff tears happen in people over the age of 30. Full-thickness rips can happen to those who are younger.
- Complaints of discomfort in the glenohumeral joint’s anterior, lateral, or posterior.
Physical Findings of Rotator Cuff Tears
Physical Findings may include:
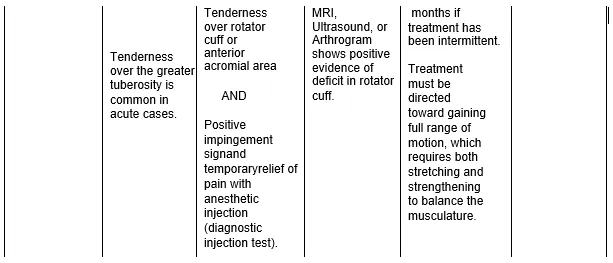
Partial-Thickness Tears
- Full passive range of motion for abduction, elevation, and external rotation will cause pain at the conclusion of the range of motion; internal rotation is possible;
- Abduction, external rotation, internal rotation, and forward flexion will all have a restricted and painful active range of motion;
- Active elevation may cause a painful arc;
- Resisted tests (abduction, flexion, external rotation, internal rotation, abduction/internal rotation at 90 degrees, and abduction/external rotation at 45 degrees) will result in pain; alternatively, they may not.
- Refer to Section D.6, Impingement Syndrome, if there are positive impingement indications.
Full-Thickness Tears of Rotator Cuff Tears
- Similar to partial-thickness tears in terms of passive and resisted findings; and/or
- Active elevation will be significantly constrained, and scapular rotation will clearly take its place.
Laboratory Tests of Rotator Cuff Tears
Laboratory Tests of Rotator Cuff Tears is recommended – When a systemic illness or disease is suspected in a subset of patients.
Testing Procedures X-ray of Rotator Cuff Tears
Testing Procedures X-ray of Rotator Cuff Tears is recommended – Clinically appropriate in a subset of patients. X-Rays \sinclude:
- A tear in the rotator cuff can be seen in the AP view as elevation of the humeral head, which indicates a long-standing injury;
- Anterior or posterior dislocation, as well as the existence of a defect in the humeral head (a Hill-Sachs lesion), are determined by a lateral view in the plane of the scapula or an axillary view;
- If there is a spur on the anterior/inferior surface of the acromion and/or the far end of the clavicle, it can be seen in a 30 degree caudally angulated AP view;
- Outlet view indicates whether an acromion with a downward tip exists.
Adjunctive Testing (Sonography, Arthrography or MRI) of Rotator Cuff Tears
Adjunctive Testing (Sonography, Arthrography or MRI) of Rotator Cuff Tears is recommended – Clinically appropriate in a subset of patients.
Indications: When non-operative conservative treatment for shoulder discomfort fails after four to six weeks and the diagnosis cannot be made by using normal radiography techniques, sonography, arthrography, or MRI may be advised. When there is a clinical suspicion of a full-thickness rotator cuff tear, an MRI should be done sooner (for example, within one to two weeks).
Non-Operative Treatment Procedures of Rotator Cuff Tears
Nonsteroidal anti-inflammatories and analgesics would be recommended, and an acute rotator cuff tear might need the use of some narcotic painkillers.
Rest and non-surgical treatments such immobilisation, therapeutic exercise, changing one’s job or work station, thermal treatment, and therapeutic ultrasound. When shoulder pain is acute, passive modalities should only be used during the first two to three weeks. Active therapies should then be added as soon as they are NYS WCB MTG – Shoulder Injury 47 suitable.
After sufficient participation in a rehabilitation programme, a surgical consultation is necessary if no clinically significant improvement in function for a partial- or full-thickness tear is seen. Adequate in this context is defined as a minimum of two to three sessions per week for four weeks in an active physical therapy programme with at least 75% attendance.
A physical therapy regimen that only employs passive methods or for which the claimant hasn’t shown evidence of compliance is insufficient. Early surgical intervention results in improved surgical outcomes because of stronger tissues and frequently fewer postoperative movement restrictions.
Operative Procedures
Post-Operative Procedures of Rotator Cuff Tears
- A customised rehabilitation plan based on interaction between the doctor, the surgeon, and the therapist might include:
- Abduction splint or sling;
- To avoid adhesions and preserve mobilisation, use gentle pendulum exercises and passive glenohumeral range of motion in flexion and external rotation;
- Start engaging in isometrics and ADLs six weeks after surgery;
- Active aided supine range of motion leading to sitting
- Start modest resistance exercise at six to eight weeks, depending on the tissue quality;
- Scapular mobilisation exercise with glenohumeral stabilisation, manual resistive exercise at 90 degrees, and
- Exercise for the scapular plane.
- Pool Exercise
- Between three and six months of progressive resistance training, followed by a gradual return to full activity between six and nine months. Consideration should be given to all active non-operative procedures described in Section E, Therapeutic Procedures: Non-Operative.
- During the post-operative recuperation and rehabilitation, work limits should be assessed every four to six weeks with appropriate written notifications to the patient and employer. If the patient’s progress stagnates, the provider should reassess the patient’s health and modify the treatment plan as necessary.
What our office can do if you have Rotator Cuff Tears
We have the experience to help you with their workers compensation injuries. We understand what you are going through and will meet your medical needs and follow the guidelines set by the New York State Workers Compensation Board.
We understand the importance of your workers compensation cases. Let us help you navigate through the maze of dealing with the workers compensation insurance company and your employer.
We understand that this is a stressful time for you and your family. If you would like to schedule an appointment, please contact us so we will do everything we can to make it as easy on you as possible.
