The New York State workers compensation board has developed these guidelines to help physicians, podiatrists, and other healthcare professionals provide appropriate treatment for History Taking and Physical Examination of Mid and Low Back Injury.
These Workers Compensation Board guidelines are intended to assist healthcare professionals in making decisions regarding the appropriate level of care for their patients with ankle and foot disorders.
The guidelines are not a substitute for clinical judgement or professional experience. The ultimate decision regarding care must be made by the patient in consultation with his or her healthcare provider.
History Taking and Physical Examination of Mid and Low Back Injury
Physical examination and history-taking lay the groundwork for and direct the progression of diagnostic and therapeutic procedures. When results from clinical assessments and those from other diagnostic techniques are: When two things are inconsistent with one another, objective clinical findings are more important.
The following should be appropriately documented in the medical records:
History of Present Illness
Evaluation and therapy should be mostly based on a thorough history obtained shortly after the accident. The background should contain:
- Details on the onset and development of symptoms are included in the mechanism of injury. The mechanism of injury should include a thorough account of the incident and the body’s position before, during, and after the incident. In the absence of a specific occurrence, considerations such as frequency during the workday, lifting/push/pull requirements, and body postures at work should be taken into account.
- Location, type, and circumstances that either lessen or exacerbate your pain (e.g., sitting tolerance). Primary back pain, secondary hip pain, and groin pain, for example, should all be mentioned in history.
- To ensure that all work-related symptoms, including pain, are also being addressed, it is highly suggested to adopt a recognized pain assessment tool (e.g., the Visual Analog Scale [VAS]), particularly during the first two weeks after injury.
- Lower extremity numbness, tingling, or weakness, particularly if brought on by or exacerbated by sneezing or coughing.
- Prior injuries, both occupational and non-occupational, to the same area, including specific prior treatment, a history of particular prior auto accidents, persistent or recurring symptoms, and any functional restrictions review of any earlier imaging examinations of the spine.
- Previous emotional and/or psychological responses to the accident or sickness at hand.
- Ability to carry out regular tasks and job responsibilities.
Past History
- whole medical history from the past.
- It is important to conduct a system review, which may include signs or symptoms from the following organ systems: integumentary/breast; neurological; psychiatric; hematologic/lymphatic; allergic/immunologic; constitutional symptoms; eyes; ear, nose, and throat; cardiovascular; respiratory; gastrointestinal; genitourinary; musculoskeletal; The scope and focus of the assessment of systems can vary from case to case depending on the underlying ailment being treated and clinical judgment.
- smoking history
- both professional and recreational activities.
- Previous experience with depression, anxiety, or another mental disorder.
Physical Examination
Using the medical history as a guide, the exam should use recognized tests and techniques appropriate to the area being checked, such as:
- Vital signs,
- General examination, including posture, stance, and gait
- Visual inspection, and
- Vital signs
- Palpation
- Lumbar mobility, quality of movement, and presence of muscular cramping Motion analysis of particular joints could be indicated.
- Thoracic spine and pelvis examination
- Nerve pressure testing, When the Capri Length Lasegue Test When a raise test) is conducted, a result is typically not thought to be optimistic at altitudes of less than 25 or more than 60 degrees (and the degrees should be always reported).
- Study of the lower extremities’ sensory and motor function with a focus on certain nerve roots.
- Deep tendon reflexes.
- If necessary, perform an abdominal exam, measure the circumference of the lower extremities, or check for other abnormalities of the lower extremities.
- The hip should be examined for ROM, discomfort, deformity, etc.
- Palpation of the distal pulses is part of the lower extremity vascular examination.
Spinal Cord Evaluation
Additional investigation is needed when the injury, epidemiology, or clinical condition points to a potentially serious injury. Among the many neurological tests for potential spinal cord damage are:
- temperature, temperature contrast, deep pressure, and proprioceptive sensory function;
- Strength testing;
- Pathological reflexes and anal sphincter tone and/or perianal sensation are present.
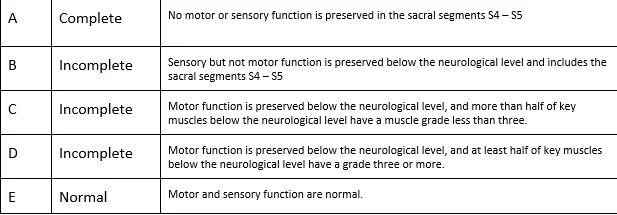
- According to the American Spine Injury Association (ASIA) impairment scale, spinal cord lesions should be categorized.
- Spinal cord lesions should be classified according to the American Spine Injury Association (ASIA) impairment scale.
ASA Impairment Scale
Red Flags
Red flags are observations that suggest potentially significant and urgent medical issues. The review of the history and physical examination should include looking for warning signs. Acute fractures, dislocations, infections, tumors, increasing neurologic deficits or cauda equina syndrome, and extraspinal illnesses are a few examples of these observations or signs in the mid and low back.
The New York Mid and Low Back Injury Guidelines contain modifications in clinical management brought on by the existence of “red flags,” and further evaluation/consultation or urgent/emergent action may be necessary.
What our office can do if you have workers compensation History Taking and Physical Examination of Mid and Low Back Injury
We have the experience to help you with their workers compensation injuries. We understand what you are going through and will meet your medical needs and follow the guidelines set by the New York State Workers Compensation Board.
We understand the importance of your workers compensation cases. Let us help you navigate through the maze of dealing with the workers compensation insurance company and your employer.
We understand that this is a stressful time for you and your family. If you would like to schedule an appointment, please contact us so we will do everything we can to make it as easy on you as possible.
