The New York State workers compensation board has developed these guidelines to help physicians, podiatrists, and other healthcare professionals provide appropriate treatment for Hip and Groin Disorders.
These Workers Compensation Board guidelines are intended to assist healthcare professionals in making decisions regarding the appropriate level of care for their patients with ankle and foot disorders.
The guidelines are not a substitute for clinical judgement or professional experience. The ultimate decision regarding care must be made by the patient in consultation with his or her healthcare provider.
Diagnostic Approach of Occupational Interstitial Lung Disease
The diagnosis of occupational ILD is typically made clinically, taking into account the occupational history of sufficient exposure with the appropriate latency, objective radiographic evidence (chest radiograph and/or HRCT), assessment of pulmonary function (including consistent changes in ventilatory capacity, static lung volumes, or gas exchange), and consideration of other differential diagnoses.
Lung biopsy is infrequently required to make the diagnosis of occupational ILD in a worker with a typical clinical picture (containing exposure history, latency, and radiographic presentation).
It may occasionally be necessary to perform a pathologic investigation of lung tissue when the clinical or radiographic characteristics are ambiguous or unusual.
Recommended: Follow-Up Diagnostic Tests
In the medical assessment of pulmonary occupational disease, periodic medical follow-up is necessary. This includes imaging scans and lung function testing.
Spirometry of Diagnostic Testing
A good initial test for lung function is spirometry. Spirometry distinguishes between obstructive and restrictive lung patterns of lung function and provides physiologic evidence for occupational ILD. All patients should undergo spirometry as a critical step in the diagnosis and follow-up of occupational interstitial lung disease.
Spirometry, however, does not identify ILD. According to recognised ATS recommendations, abnormal spirometry results should prompt additional testing, including confirmation by lung volume assessment, or a referral to a specialist.
Measuring lung volumes and diffusing capacity should ideally be a part of the contemporary diagnostic evaluation of pulmonary occupational illness. In addition to the diagnostic and therapeutic evaluations of occupational lung illness, further research on gas exchange physiology, cardiopulmonary exercise testing, and/or the six-minute walk test should be employed when clinically necessary.
Diagnostic spirometry testing technique:
- Should be carried out by a technician who has the necessary training, using the recommended tools and techniques.
- Should be carried out in line with the American Thoracic Society’s most recent recommendations or specifications, as well as those of OSHA, NIOSH, and the Mine Safety and Health Administration (MSHA).
- When diagnostic spirometry results are abnormal, testing should be performed again as soon as practical to make sure the worker was inhaling as deeply as possible, blowing out forcefully, and exhaling completely throughout the test.
- The most common way to determine whether short-term reversibility of the spirometry results can be reversed is to repeat the test after the subject has gone through a prescribed short-acting bronchodilator inhalation protocol if the results are still abnormal.
- The diagnostic interpretation may compare the worker’s highest results with normal ranges derived from suitable similar groups once an acceptable test has been recorded for the individual.
Interpretation – The examination of workers at risk of occupational ILD includes a number of procedures, including the interpretation of spirometry tests. First, the interpreter must assess test quality, offer feedback, and decide whether acceptability standards have been fulfilled.
Adjust for age, height, gender, and race/ethnicity using the proper reference tables for normal or projected values if the test is deemed acceptable for interpretation.
Patients who have previously undergone spirometry have their test results monitored over time for changes.
Spirometry for the Diagnosis and Monitoring of Occupational Interstitial Lung Disease
Spirometry of Diagnostic Testing
- Spirometry of Diagnostic Testing is recommended when diagnosing and keeping track of people with interstitial lung illnesses brought on by their jobs.Indications – Diagnostic criteria include patients having a history of ILD and/or chest radiography that supports the diagnosis, as well as workplace exposure that supports plausible etiologies (e.g., a worker complaining of a persistent or sporadic cough, shortness of breath, or diminished physical capabilities). In general, spirometry should be postponed in cases of recent surgery, respiratory illnesses, or heart issues.Indications – Monitoring/Surveillance: For workers in occupations with exposures that are either known or suspected to be related with the development of occupational lung disease, periodic spirometry (yearly) with longitudinal examination of loss of pulmonary function is advised.Monitoring FEV1 decline over time allows for longitudinal study. since the most reproducible lung function parameter, the FEV1, is time. Calculating such an evaluation should be done when The technical quality of spirometry testing is adequate.In general, a decline in FEV1 greater than 50 ml/year is regarded as a pulmonary function loss that exceeds the ageing impact. The National Institute of Occupational Safety and Health (NISOH), American Thoracic Society (ATS), and American College of Occupational Medicine (ACOEM) have all proposed various methodologies to calculate the loss of pulmonary function and determine whether such loss is greater than the expected age-related loss of pulmonary function.Trends over time can be calculated using computer software, such as Spirola from NIOSH.
Static (Full) Lung Volumes of Diagnostic Testing
When additional diagnosis clarification is required, measurement of static lung volumes, such as Total Lung Capacity (TLC), Functional Residual Capacity (FRC), and Residual Volume (RV), is recommended to supplement the results of a spirometry test.
Spirometry results showing a decreased FVC could result from a number of different illness processes. Measurement of static lung volumes is necessary to validate the diagnosis of a truly restrictive disease, i.e., a lowered TLC below lower limits of normal, in order to properly explain a reduced FVC on spirometry.
For example, in emphysema or asthma, static lung volumes can be utilised to determine whether air trapping is present in obstructive disorders. The RV/TLC ratio and the TLC are both higher under these circumstances.
The static lung volumes can be measured using body plethysmography or inert gas dilution.
- Static (Full) Lung Volumes of Diagnostic Testing
Static (Full) Lung Volumes of Diagnostic Testing is recommended To explain a lower FVC on spirometry, particularly when the FEV1/FVC ratio is normal, in the assessment of occupational ILD.Indications – In particular, when the FEV1/FVC ratio is normal, static lung volumes are advised in the assessment of occupational ILD to shed light on a lower FVC on spirometry.
Measurement of Oxygenation of Diagnostic Testing
An arterial blood gas sample or non-invasive oximetry can be used to measure oxygenation.
Oxyhemoglobin, or the oxygen saturation of the hemoglobin, is measured by non-invasive oximetry. It is an easy technique that is frequently used in an outpatient setting.
Alveolar-arterial oxygen gradient can be calculated using arterial blood gas and is useful for precisely determining the partial pressure and saturation of oxygen.
Measurement of Oxygenation of Diagnostic Testing
- Measurement of Oxygenation of Diagnostic Testing is recommended Pulse oximetry is a non-invasive method of measuring oxygenation used in the diagnosis and treatment of occupational ILD.
- Measurements of Oxygenation of Diagnostic Testing are recommended Indications Measurements of oxygenation are recommended in the assessment of Occupational ILD.
Indications – Oxygenation measurements are advised in the evaluation of occupational ILD.
Chest Radiographs of Diagnostic Testing
Imaging tests should be part of the evaluation of pulmonary occupational illness. A chest radiograph PA and Lateral should be the absolute minimum of the diagnostic process. It is preferred to interpret chest radiographs for pneumoconiosis in accordance with the International Labor Organization Classification.
In addition to providing information on the level of involvement and disease progression, radiographs provide structural anatomic information about the lung parenchyma and pleura that aids in the differential diagnosis of occupational ILD.
Radiographs, while useful in the identification of occupational lung disorders, lack the sensitivity and specificity of CT/HRCT.
In order to diagnose ILD and occupational lung disease, radiographs should be evaluated by a doctor with the necessary education, experience, and expertise. It is preferable for readers who have “B” reader certification for this classification system or people with the necessary education and experience to interpret radiographs in accordance with the International Labour Organization (ILO) classification(80) in order to document the patterns and severity of radiographic appearances of pneumoconiosis.
The Board is aware that other standard-setting bodies occasionally demand “B” reader qualifications for radiological interpretation.
- Posterior-Anterior (PA) and Lateral Chest Radiographs
Posterior-Anterior (PA) and Lateral Chest Radiographs are recommended for determining the cause of work-related interstitial lung disease.Performed – It is recommended that medical professionals who interpret chest x-rays for the diagnosis of occupational lung illness possess the necessary education, training, and expertise. They should also be certified as “B” readers under the ILO categorization system.
High Resolution Computed Tomography (HRCT) Scans /Computed Tomography (CT)
When additional diagnostics are necessary for the diagnosis of occupational ILD based on clinical findings, HRCT/CT should be taken into consideration (including spirometry and chest X-Ray). Readers of HRCT/CT images for occupational lung illness should possess the necessary knowledge and skills. A thoracic radiologist with specialist training should examine the chest CT image.
HRCT/CT
- HRCT/CT is recommended in order to confirm or rule out an ILD diagnosis during the assessment of occupational ILDIndications/Technique: In order to confirm or rule out a diagnosis of occupational ILD, HRCT/CT may be useful.
- Lung, mediastinal, and high-resolution windows should be included in HRCT/CT of the chest where warranted.
- HRCT/CT is often conducted while the patient is supine, although in some cases, such as when confirming that mild peripheral and/or basilar results are indicative of interstitial abnormalities, prone imaging may be helpful.
- When examining air trapping linked to HP, inhalatory/expiratory imaging is especially helpful.
HRCT/CT is recommended As this imaging study not only has diagnostic value but can also be used as a screening test for early detection of lung cancer, it can be used in the diagnostic workup of pneumoconiosis and other pulmonary occupational diseases, particularly in those lung diseases that result in increased risk for lung cancer.
Magnetic Resonance Imaging (MRI) of the Chest
- Magnetic Resonance Imaging (MRI) of the ChestMagnetic Resonance Imaging (MRI) of the Chest is not recommended as a major instrument for detecting occupational ILD
PET/CT Scans of the Chest
- PET/CT Scans of the Chest
PET/CT Scans of the Chest is recommended in select cases in the evaluation of cancer associated with ILD (lung cancer and mesothelioma) and certain other comorbid conditions.
Carbon Monoxide Diffusing Capacity (DLco)
The DLco test (Diffusing capacity of the lungs) gauges the flow of gas from the lungs’ alveoli and air gaps to the blood coursing via the pulmonary capillaries. The single breath diffusing capacity test, which gauges this diffusion, is referred to as DLco.
A specified amount of CO is breathed by the patient during this test, and the difference between what is inhaled and the CO detected in the exhaled gas is calculated as the lung’s capacity to diffuse a gas into blood.
Through the use of a calibrated test gas, CO, the test evaluates the lungs’ capacity to deliver oxygen to blood in an indirect manner.
The test can be used to evaluate lung function and the existence of numerous lung disorders, including ILD, by using the right test procedures and result adjustments.
The test should be conducted in accordance with the 2017 ATS/ERS statement. This claim outlines the procedures and modifications that must be carried out in order to provide a reliable test.
Further:
- The average of at least two DLco tests should be reported.
- The two DLco measurements must agree within 10%.
- It’s crucial to find out if a person smokes, as doing so may result in quantifiable baseline CO levels that increase back pressure and carboxyhemoglobin.
- The patient’s haemoglobin must be on hand because anaemia will reduce the measured diffusion. There are equations available for correcting anaemia.
Carbon Monoxide Diffusing Capacity (DLco)
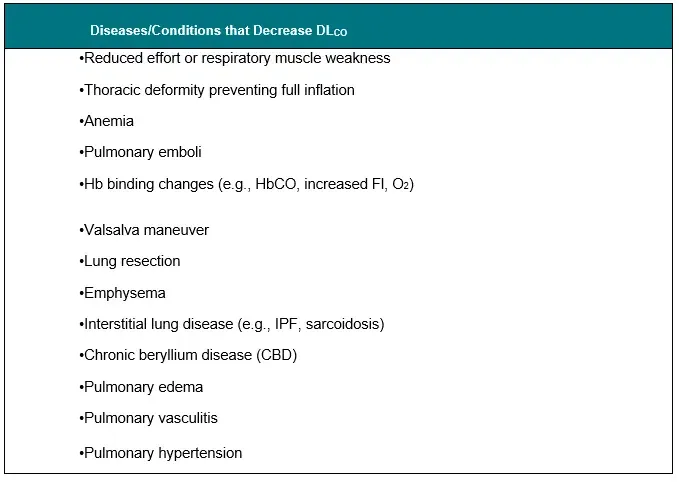
- Carbon Monoxide Diffusing Capacity (DLco)Carbon Monoxide Diffusing Capacity (DLco) is recommended to be used in the analysis of occupational lung illness.Indications – In patients with lung disease, DLCO may be utilised to aid in the diagnosis of anomalies in gas exchange.Advantages and Limitations – DLC may be impacted by a variety of ailments and exposures (Table 3). When interpreting the test findings, these need to be taken into account.
Table 3. Diseases /Conditions Associated with Alterations in DLCO
Biological Sampling of Diagnostic Testing
Invasive Procedures
Although bronchoscopy, bronchoalveolar lavage analysis, and lung biopsy are not always necessary to diagnose occupational lung illness, they should be part of the diagnostic toolbox when they are clinically indicated and/or required to confirm or rule out a particular diagnosis. In several illnesses, specific CT findings are frequently regarded as diagnostic.
Sputum Samples and Bronchoalveolar Lavage (BAL)
Additional testing, such as biological sampling, may be necessary to confirm the diagnosis of occupational ILD if the objective clinical evidence from the physical examination, chest radiography, and spirometry is insufficient.
- Sputum Sample (both induced and spontaneous)Sputum Sample (both induced and spontaneous) is recommended as a tool for the diagnosis of occupational lung illness in a subset of individuals.Indication/Technique – Additional testing, such as sputum sampling, may be necessary to confirm the diagnosis of occupational ILD if insufficient clinical objective evidence is discovered through physical examination, chest radiography, and spirometry.Given the availability of contemporary testing, such as HRCT, sputum sampling may support the diagnosis of occupational lung disease but is not strictly necessary.In order to collect a sample, the patient is made to cough in an effort to release sputum from the patient’s deep lungs. Each sample should be at least 15 mL in volume in order to improve the sample’s sensitivity.
- Bronchoalveolar Lavage
Bronchoalveolar Lavage is recommended as a tool for the diagnosis of occupational lung illness in a subset of individuals.Indications/Technique – to aid in the detection of interstitial lung disease associated with employment. Given the availability of contemporary testing, BAL may help with the diagnosis but is not necessary (i.e. HRCT).The ATS guidelines for performing BAL for ILD should be followed when performing BAL.
Bronchoscopy and/or Lung Biopsy
Bronchoscopy and/or Lung Biopsy is recommended in a small number of individuals to confirm or rule out a diagnosis in particular situations
What our office can do if you have workers compensation injuries
We have the experience to help you with their workers compensation injuries. We understand what you are going through and will meet your medical needs and follow the guidelines set by the New York State Workers Compensation Board.
We understand the importance of your workers compensation cases. Let us help you navigate through the maze of dealing with the workers compensation insurance company and your employer.
We understand that this is a stressful time for you and your family. If you would like to schedule an appointment, please contact us so we will do everything we can to make it as easy on you as possible.
We are orthopedic surgeons and do not treat chest diseases. We will refer you to someone in your area who does treat respiratory symptoms.