Partial and total knee replacement are surgical treatments used to relieve pain and disability from knee arthritis. Both procedures replace damaged parts of the knee with artificial metal and plastic components. The main difference is how much of the knee joint is replaced. A partial knee replacement treats only one knee compartment, while a total knee replacement replaces all compartments.
How Common It Is and Who Gets It? (Epidemiology)
Knee replacement is a common surgery for people with severe arthritis. Many older adults have the procedure, and more younger patients are choosing it as newer implants last longer. Partial knee replacement is less common than total knee replacement because fewer patients meet the strict criteria for it.
Why It Happens – Causes (Etiology and Pathophysiology)
Osteoarthritis is the main cause of knee replacement. The smooth cartilage that protects the bones wears down over time. This leads to pain, stiffness, swelling, and deformity of the knee. In some people, arthritis affects only one part of the knee. In others, it affects the whole joint, making a total knee replacement necessary.

X-ray showing a partial knee replacement.
How the Body Part Normally Works? (Relevant Anatomy)
The knee joint has three compartments: the inner (medial), outer (lateral), and front (patellofemoral). Healthy cartilage covers the bones and allows smooth movement. Ligaments, the meniscus, and surrounding muscles help stabilize the joint. When cartilage and bone wear down, the joint becomes painful and may lose its normal motion.
What You Might Feel – Symptoms (Clinical Presentation)
People with knee arthritis often feel pain, stiffness, swelling, and trouble walking or climbing stairs. They may notice deformity such as bow-legs or knock-knees. Pain may worsen with activity and improve with rest. Some patients lose the ability to fully bend or straighten the knee.
How Doctors Find the Problem? (Diagnosis and Imaging)
Diagnosis includes a review of symptoms, physical exam, and imaging studies. X-rays show cartilage loss, bone damage, and deformity. This helps determine whether arthritis affects one compartment or the entire knee, guiding the decision between partial and total replacement.
Classification
Knee arthritis is classified by which compartments are affected and by the severity of wear.
- One-compartment arthritis may be treated with partial knee replacement.
- Multiple-compartment arthritis usually requires total knee replacement.
Ligament stability, meniscus condition, and knee alignment also play a role.
Other Problems That Can Feel Similar (Differential Diagnosis)
Conditions that can mimic knee arthritis include ligament injuries, meniscus tears, tendon irritation, bursitis, and inflammatory joint diseases. These must be ruled out before recommending surgery.
Treatment Options
Non-Surgical Care
Before surgery, patients may try physical therapy, injections, braces, weight management, and pain medications. Surgery is offered only when these methods no longer help.
Surgical Care
Partial knee replacement replaces only one worn compartment. The surgeon uses a smaller incision and removes only the damaged bone surfaces. Ligaments and other soft tissues remain intact. This allows more natural knee motion and quicker recovery.
Total knee replacement removes the worn surfaces in all three compartments. The bone ends are shaped so metal parts fit securely, with a plastic insert in between. This is recommended when arthritis affects more than one compartment or when the knee has deformity, ligament damage, or meniscus problems.
Partial knee replacement
In a partial knee replacement, only one of the compartments of the knee is replaced. During a partial knee replacement surgery, the surgeon accesses the joint through a usually smaller incision. The diseased ends of the bones forming the compartment are then cut to be removed. All the ligaments and other soft tissue structures are left intact.
A metal prosthetic component is placed on the cut bony ends and fixed with bone cement. A high-grade plastic part is placed in between the metal parts for the smooth gliding of the metal surfaces. The incision is closed in layers and the patient is able to walk the same day of the surgery.
Not all patients are candidates for partial knee replacement. The partial replacement surgery is only recommended in the following patients:
- Patients with evidence indicating the involvement of only one compartment of the knee joint.
- The knee joint is stable without any damage to the ligaments such as the anterior cruciate ligament, posterior cruciate ligament, or medial and lateral collateral ligaments.
- Patients with no history of meniscus surgery in the other compartment.
- Generally, patients with less demanding lifestyles
- Patients with who are not in the obese BMI category.
- Patients with no evidence or history of inflammatory arthritis such as rheumatoid arthritis, reactive arthritis, etc.
- Patients with no significant deformity of the knees such as bow legs, knock knees, flexion deformities, or inability to bend the knee more than 90 degrees.
Partial vs Total Knee
Since the partial knee replacement involves the replacement of only one of the knee compartments, the surgery time is significantly less than the total knee replacement. The risk of complications associated with a knee replacement surgery such as blood loss, nerve damage, deep vein thrombosis, infection, etc is also less in the case of a partial knee replacement.
Since less tissue and bone are cut and the ligaments are left intact, a partial knee replacement has a more natural feeling to the knee joint. Comparatively, patients who undergo total knee replacement often complain of feeling unnatural mechanical knees. The unnatural feeling often a results of loss of proprioception. These are sensory nerves that reside in ligaments, and provide information to the brain regarding your limb’s position in 3D space. These ligaments are sacrificed in total knee replacements. As a result the knee provides less proprioception information to the brain, and the knee can feel “unnatural”.
Patients undergoing partial knee replacement are able to get back to their daily activities sooner than total knee replacement. As significantly less cutting is involved in a partial knee replacement, the patients experience less postoperative pain and are able to participate in rehabilitation sooner.
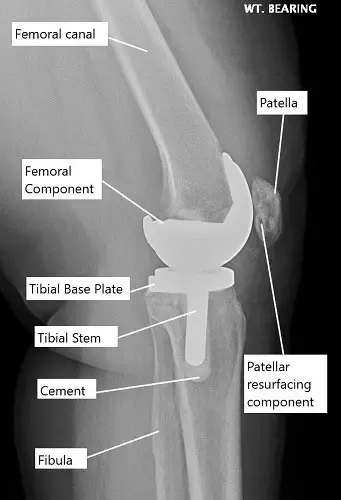
X-ray showing a total knee replacement.
Partial knee replacement however is not frequently done even in patients with unicompartmental knee arthritis as:
- In the majority of cases, a partial knee replacement may need revision surgery in the form of a complete knee replacement. Arthritis eventually may involve the other compartments of the knee causing pain and deformity.
- The revision surgery to total knee replacement from a partial joint replacement is often more complicated than a primary total knee replacement surgery.
- A number of patients with knee arthritis have deformities such as knock knees, bow-legs, or inability to completely straighten or bend the knee. The deformity can be easily corrected in a total knee replacement leading to better knee kinematics.
- Any subsequent ligament or meniscus damage in a patient with a partial knee replacement surgery may require a revision into a total knee replacement.
- Inflammatory arthritis usually involves the entire joint instead of a single compartment. Patients with inflammatory arthritis are more effectively managed with a total knee replacement surgery.
Total knee replacement surgery has revolutionized the management of knee arthritis. Patients today prefer an early joint replacement surgery after failure of non-surgical methods due to the drastic improvement in quality of life with regained mobility.
The majority of the patients who may be candidates for a partial knee replacement generally opt for a total knee replacement due to lower revision rates.
Decision Factors for PKR vs. TKR
The choice between PKR and TKR often depends on several factors:
- Extent of arthritis: TKR is necessary if multiple compartments of the knee are affected.
- Patient’s age and activity level: Younger, more active patients may benefit from the natural knee feel of a PKR, whereas older patients with less demanding daily activities might be better candidates for TKR.
- Overall health: Patients with other health issues might opt for PKR to reduce the time under anesthesia and minimize hospital stay.
Recovery and What to Expect After Treatment
Recovery for both surgeries includes walking the same day or the next day and starting early physical therapy. Most people return to daily activities sooner after partial knee replacement because less bone and tissue are removed. Full recovery can take several months. Regular therapy helps restore strength, motion, and balance.
Possible Risks or Side Effects (Complications)
Risks include infection, blood clots, bleeding, nerve injury, and stiffness. Partial knee replacement has lower risks because less tissue is cut. However, partial replacements may need revision later if arthritis spreads to other compartments. Revision from partial to total knee replacement can be more complex than performing a first-time total knee replacement.
Long-Term Outlook (Prognosis)
Both surgeries offer excellent long-term outcomes. Many patients experience major pain relief and improved mobility. Total knee replacement has lower revision rates and is preferred by most patients once they qualify for surgery. Partial knee replacement feels more natural but may not last as long because arthritis can develop in the remaining compartments.
For insurance and cost information, see our Insurance Information page.
Frequently Asked Questions (FAQ)
Q. Which surgery feels more natural?
A. Partial knee replacement often feels more natural because the ligaments are kept intact.
Q. Which surgery lasts longer?
A. Total knee replacement has lower revision rates. Partial replacements may need revision if arthritis spreads.
Q. Who is a good candidate for partial knee replacement?
A. People with arthritis in only one compartment, stable ligaments, and no major deformity.
Q. Which option has a faster recovery?
A. Partial knee replacement usually has a quicker early recovery.
Q. Can partial knee replacement be converted to total knee replacement later?
A. Yes, but the revision surgery is more complex than a first-time total knee replacement.
Summary and Takeaway
Partial knee replacement treats arthritis in one compartment and offers quicker recovery and a more natural knee feel. Total knee replacement treats arthritis in all compartments and has lower revision rates and broader use. The choice depends on how many parts of the knee are affected, ligament stability, deformity, and the patient’s lifestyle. Both options offer strong pain relief and improved movement.
Clinical Insight & Recent Findings
A recent study evaluated ways to improve recovery after total knee replacement and found that patients experienced less postoperative pain and required fewer opioids when standard care was supplemented with a digital education app and enhanced physician communication, compared with routine treatment alone .
Although this research focused on total knee replacement, its findings reinforce key principles relevant when comparing partial and total knee replacement: patient experience, pain control, and functional recovery depend not only on the extent of surgery but also on perioperative support, expectation management, and tailored care.
These results align with the discussion above, where partial knee replacement often offers a faster, more natural recovery due to less tissue disruption, while total knee replacement remains the more durable option when arthritis affects multiple compartments; in both cases, structured guidance and patient-centered postoperative care can significantly enhance overall outcomes. (“Study on postoperative recovery after knee replacement – see PubMed.“)
Who Performs This Treatment? (Specialists and Team Involved)
Orthopedic surgeons perform both partial and total knee replacements. They work with nurses, physician assistants, physical therapists, and anesthesiologists who guide care before, during, and after surgery.
When to See a Specialist?
You should see a knee specialist if pain, swelling, or stiffness limits daily activities, or if nonsurgical treatments no longer help. A specialist can determine whether your arthritis affects one or multiple compartments.
When to Go to the Emergency Room?
Seek emergency care if the knee becomes very swollen, hot, or red, or if you cannot walk or straighten the leg. After surgery, fever, drainage, or sudden severe pain need urgent attention.
What Recovery Really Looks Like?
Recovery includes therapy, swelling control, and steady improvement in strength and motion. Partial knee replacement often allows quicker return to activity, but both surgeries require commitment to therapy and home exercises.
What Happens If You Ignore It?
Ignoring advanced knee arthritis can lead to worsening pain, greater stiffness, deformity, and reduced ability to walk. Over time, this can limit treatment options and make recovery more difficult.
How to Prevent It?
Maintaining a healthy weight, staying active, avoiding high-impact activities, and treating injuries early can help reduce stress on the knee and may slow arthritis progression.
Nutrition and Bone or Joint Health
A balanced diet rich in protein, vitamin D, and calcium supports joint and bone health. Good hydration also helps overall recovery.
Activity and Lifestyle Modifications
Low-impact activities like cycling, swimming, and walking help keep the knee strong. Avoiding twisting, heavy lifting, and high-impact sports protects the joint and helps the replacement last longer.
Do you have more questions?
Are there any age restrictions for either PKR or TKR?
There are no strict age restrictions for either procedure. The decision is more dependent on the patient’s overall health, activity level, and the extent of joint damage rather than age alone.
How long do the implants from a PKR and TKR last?
Knee replacement implants can last 15-20 years or more, but longevity can vary based on factors like the patient’s activity level, weight, and the accuracy of the implant placement during surgery.
What is the risk of infection with knee replacement surgery?
The risk of infection is low, typically around 1-2% for knee replacements. Hospitals take numerous precautions to prevent infections, including antibiotics before and after surgery.
Can I undergo a PKR if I have had previous knee surgeries?
Yes, you can still be a candidate for PKR after previous knee surgeries, depending on the condition of your knee and the type of surgeries performed. Each case needs to be evaluated individually.
What are the signs that I might need a TKR instead of a PKR?
You might need a TKR if you have severe arthritis affecting more than one compartment of the knee, significant stiffness, or you have had previous surgeries that have not successfully alleviated pain.
What is the typical recovery time for PKR versus TKR?
Recovery can vary, but generally, patients recover faster from PKR, often resuming normal activities within 4-6 weeks. TKR recovery might take 8-12 weeks or longer.
What kind of anesthesia is used during these surgeries?
Both surgeries can be performed under general anesthesia, where you are completely asleep, or spinal anesthesia, where you are awake but numb below the waist.
Are there any non-surgical alternatives to knee replacement?
Yes, non-surgical options include weight management, physical therapy, anti-inflammatory medications, corticosteroid injections, and viscosupplementation injections.
How do I know if my arthritis is suitable for PKR?
An orthopedic surgeon can determine if your arthritis is limited to one compartment with a physical exam and imaging tests like X-rays or MRI.
What happens during TKR surgery?
In TKR surgery, all three compartments of the knee are replaced with prosthetic components to create new joint surfaces.
What is the success rate of PKR and TKR?
Both surgeries have high success rates, with many patients experiencing significant pain relief and improved mobility. Success rates can exceed 90% depending on the circumstances and the surgeon’s expertise.
Can I play sports after knee replacement?
While high-impact sports are generally not recommended after knee replacement, many patients can return to low-impact activities like swimming, cycling, and golf.
What is the risk of dislocation with PKR and TKR?
The risk of dislocation is more relevant to hip replacement. For knee replacements, the concern is not dislocation but rather implant loosening or wear over time.
How do I prepare for knee replacement surgery?
Preparation typically involves several preoperative tests, discussions about anesthesia, and possibly banking your own blood for transfusion if needed. It also involves planning for postoperative care and rehabilitation.
What are the major risks associated with knee replacement surgery?
Major risks include infection, blood clots, implant failure, and complications from anesthesia, although these are relatively rare.
How long will I stay in the hospital after surgery?
The stay can vary; PKR patients may go home the same day or after one night, while TKR patients might stay for a few days.
What is the difference in pain level post-surgery between PKR and TKR?
PKR generally results in less postoperative pain compared to TKR, as it is less invasive and preserves more of the knee’s natural structures.
How is the decision made between choosing a PKR and a TKR?
The decision is based on the extent of the arthritis, patient’s activity levels, overall knee condition, and personal health goals. This decision is made after thorough discussions with your orthopedic surgeon and after evaluating all diagnostic imaging.
How do I care for my knee after surgery?
Post-surgery knee care involves managing pain, preventing infection, attending physical therapy, and gradually increasing activity levels under the guidance of your healthcare provider.
What are the signs of complications after knee replacement surgery?
Signs to watch for include excessive swelling, redness, pain that worsens over time, any discharge from the incision site, fever, or any sudden decrease in mobility.
Can a PKR be converted to a TKR if needed in the future?
Yes, if arthritis develops in the other compartments of the knee, a PKR can be converted to a TKR. This is a common scenario and can be effectively managed with surgery.
What are the latest advancements in knee replacement surgery?
Recent advancements include the use of robotic-assisted surgery for greater precision, improvements in implant materials for increased longevity, and less invasive surgical techniques that aid in faster recovery.

