Total knee replacement (TKR) is one of the most effective surgeries to relieve pain and restore function in the knee joint, particularly in patients with osteoarthritis or joint degeneration. Traditionally, TKR has been performed using cemented prostheses, but recently, cementless total knee replacements have gained popularity. Both methods offer excellent outcomes, but they have distinct advantages and limitations that need to be carefully considered based on the patient’s needs.
How Common It Is and Who Gets It? (Epidemiology)
Knee replacement surgeries are increasingly common due to the rising incidence of knee arthritis, particularly osteoarthritis, among aging populations. It is also performed in younger individuals with severe joint damage due to trauma or conditions like rheumatoid arthritis. The decision between cemented and cementless knee replacements typically depends on factors like age, activity level, bone quality, and the extent of knee damage.
Why It Happens – Causes (Etiology and Pathophysiology)
Knee arthritis, which is the leading cause for total knee replacement, results from the deterioration of the knee’s cartilage, often due to wear and tear (osteoarthritis) or inflammatory conditions like rheumatoid arthritis. This leads to pain, swelling, and stiffness, limiting movement. When conservative treatments fail, knee replacement surgery is often recommended to restore function and alleviate pain.
In knee replacement, the worn-out cartilage and bone are removed, and prosthetic implants are inserted. The implant fixation method, whether cemented or cementless, affects the long-term performance of the knee joint.
How the Body Part Normally Works? (Relevant Anatomy)
The knee joint is a hinge joint where the femur (thigh bone) and tibia (shin bone) meet. The patella (kneecap) sits in front of this joint, helping facilitate smooth knee movements. Articular cartilage covers the ends of these bones, allowing them to glide smoothly against each other. Below the cartilage, the subchondral bone acts as a foundation for the joint. The knee is supported by ligaments, such as the ACL, PCL, MCL, and LCL, which provide stability during movement.
What You Might Feel – Symptoms (Clinical Presentation)
Patients with knee arthritis or severe joint damage typically experience:
- Pain: Constant or intermittent pain in the knee, especially during weight-bearing activities.
- Stiffness: Difficulty bending or straightening the knee.
- Swelling: The knee may become swollen, particularly after activity.
- Instability: A feeling of the knee “giving way” or difficulty supporting weight, often prompting patients to seek knee replacement surgery when conservative treatments no longer work.
How Doctors Find the Problem? (Diagnosis and Imaging)
The diagnosis of knee arthritis or joint degeneration is made based on clinical examination, patient history, and imaging studies:
- X-rays: The first line of imaging to assess the extent of cartilage loss, joint space narrowing, and deformities.
- MRI: Provides detailed images of the soft tissues, cartilage, and ligaments, often used to assess the severity of joint damage.
- CT Scan: May be used for detailed views of joint alignment, especially in complex cases.
Classification
Knee arthritis is classified based on its severity:
- Grade 1 (Mild): Slight narrowing of the joint space and mild symptoms.
- Grade 2 (Moderate): Moderate narrowing with some cartilage loss and worsening pain.
- Grade 3 (Severe): Significant cartilage loss, joint deformity, and daily pain.
- Grade 4 (End-stage): Total loss of cartilage with exposed bone and constant, debilitating pain.
Other Problems That Can Feel Similar (Differential Diagnosis)
Conditions that may present with symptoms similar to knee arthritis include:
- Meniscal Tears: Damage to the knee’s cartilage can cause pain, swelling, and instability.
- Ligament Injuries: ACL or PCL tears may result in instability, similar to arthritis.
- Patellofemoral Syndrome: Pain around the kneecap often caused by cartilage damage or misalignment.
Treatment Options
Non-Surgical Care
For patients with mild to moderate knee arthritis, non-surgical options may be effective:
- Physical Therapy: Strengthening exercises to improve joint function and reduce pain.
- Medications: NSAIDs for pain relief, corticosteroid injections for inflammation.
- Bracing: Knee braces to provide stability and offload stress on the joint.
Surgical Care
Surgery is recommended when non-surgical treatments fail, and it typically involves knee replacement. There are two primary approaches:
- Cemented Total Knee Replacement: Prosthetic components are fixed to the bone using bone cement. This method is most commonly used and offers immediate stability.
- Cementless Total Knee Replacement: Implants are press-fitted into the bone, allowing for biological fixation as the bone grows into the porous surface of the implant.
Cemented Total Knee Replacement
After the patients are medically cleared for surgery and received appropriate anesthesia, the knee joint is opened from the front. The diseased segments of the bones forming the joint are removed. Using cutting guides, bone cuts made in the femur, tibia and the patella.

Cemented TKA
After thoroughly washing the cut segments, acrylic bone cement is applied to the implants and the bone segments. The implants are then fixed to the prepared bed on the bone.
A plastic high-quality polyethylene space is attached to the tibial component to reduce friction between the implants. The acrylic cement hardens quickly providing immediate fixation.
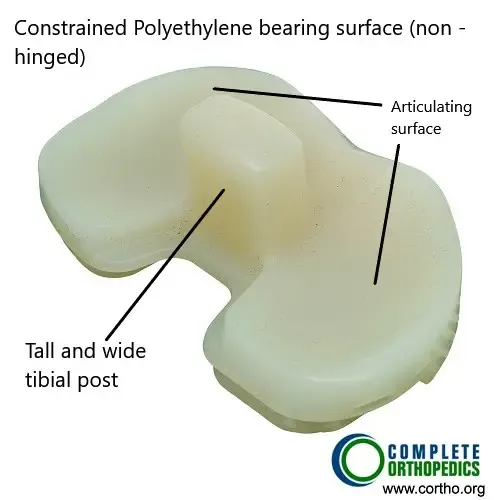
Constrained polyethylene insert
A constrained polyethylene insert may be used in a knee with ligament instability on the sides. The tall and wide tibial post on the polyethylene insert ensures rotational and small side to side stability. The insert is made of highly cross-linked polyethylene which is resistant to wear and tear. The tibial post fits in front of the femoral cam providing stability.

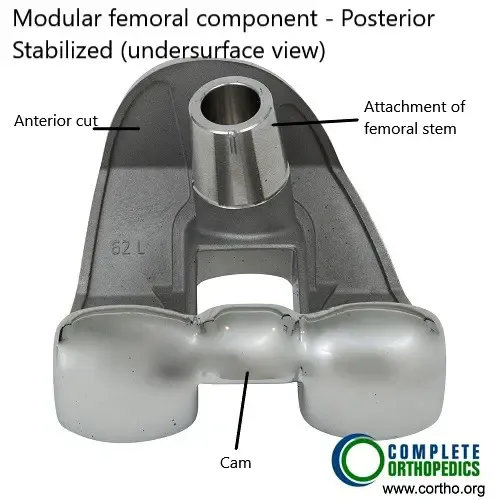
Femoral Component (posterior stabilized)
The posterior stabilized femoral component involves sacrificing the posterior cruciate ligament during surgery. The function of the posterior cruciate ligament is duplicated by the femoral cam and the tibial post mechanism.
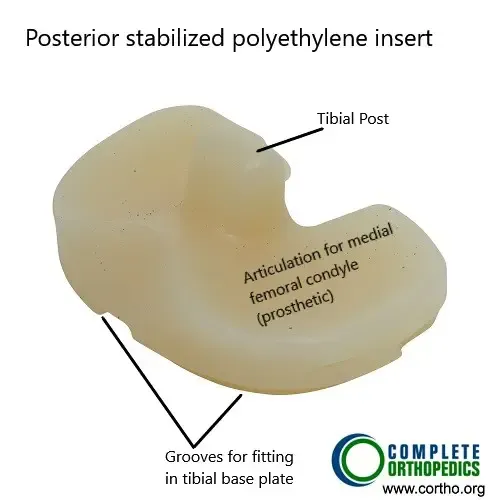
Modular femoral component
The non constrained posterior stabilized polyethylene insert has a tibial post that works along with femoral cam to provide femoral rollback. The polyethylene is highly cross linked and treated with anti-oxidants to prevent wear and particles.
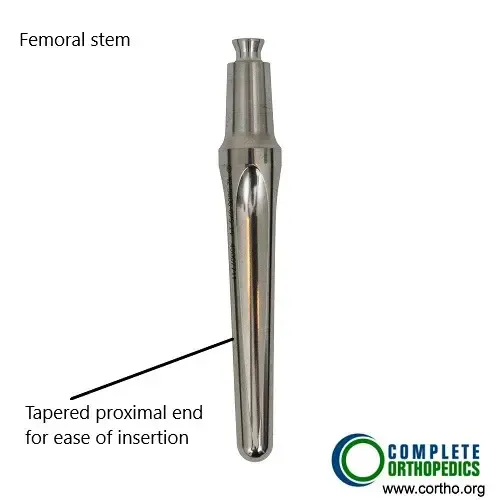
Modular femoral stem
The femoral stem fits in a modular femoral component and is used in revision surgery to achieve greater stability of the prosthesis. The stem is not cemented while the modular femoral component is cemented in the lower thigh bone.
Modular femoral component
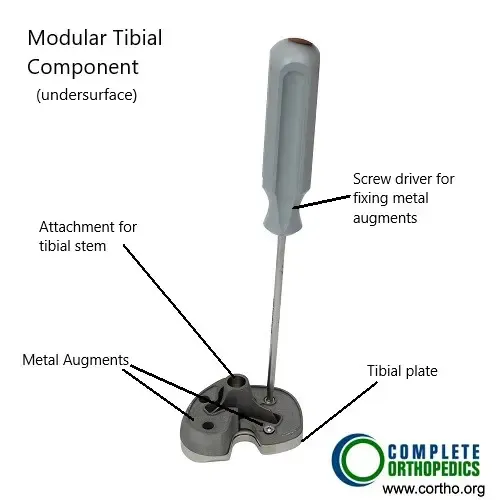
Modular tibial component with bone augments (metal wedges)
Similar to modular femoral component, a modular tibial component is used in revision knee replacement. The modular components allow attachment of stem and bone augments (metal cones/wedges) to achieve stable fixation and stabilize the prosthetic knee in all ranges of motion.
Cementless Total Knee Replacement
The surgical steps remain the same, however, the femoral and tibial components are press-fitted on the bones. The implants are specially designed to have a porous surface to allow for bone growth. The patella is cemented due to high rates of failure with cementless fixation.
The bone cuts have to be accurate in case of cementless tka for the implant to be press-fitted. Screws or pegs are used for additional fixation in case of the tibial component.
Advantages & Potential Drawbacks of Cemented Fixation
The acrylic cement dries very quickly providing immediate fixation. The cemented implants have been in use for many years now with a significant date on their success. On average, the cemented total knee prosthesis lasts for 15-20 years or more.
The cement provides excellent fixation in the case of osteoporotic or weak bones. Cemented implants provide a better fixation in old, obese, osteoporosis, cancer patients with poor bone quality.
Over a period of time, the cement which forms a layer between the bone and the implant may become loose. In younger patients, a high amount of stress on the joint may also cause loosening of the bone cement.
Once the cement begins to come loose, the implant loosens and may rub against the bone causing pain. Loosened implants frequently require revision surgery. The revision surgery is also complicated by the presence of cement.
The cement may also cause third body wear. Small fragments of the cement may break in and rub against the implants. The particles may also lead to inflammation as the body tries to remove the debris.
This may lead to a condition known as osteolysis as the inflammatory cells may also remove the bone around the implant. The loosened implant may again require revision.
As the bone cement hardens, it releases a lot of thermal energy. The heat may damage the underlying bone surface causing thermal necrosis. Additionally, the process of cementing may lead to increased chances of fat embolism.
Advantages & Disadvantages of Cementless Fixation
Cementless implants are press-fitted into the bone, as they have a special porous surface to stimulate bone growth. The bone growth happens over a long period of time thus not providing immediate fixation. As they promote biological fixation, they are proposed to have longer survivorship.
The limitations of cement fixation are not present in cementless fixation. The cementless fixation although needs good bone stock. Young patients with good bone metabolism are the ideal candidate for cementless fixation.
However, cementless fixation requires accurate bone cuts to prevent any gaps between the implant and the bone surface. The surgery time for cementless fixation is significantly less than the cemented fixation. The chances of osteolysis are reduced in cementless fixation but the microscopic particles from the implant may still lead to osteolysis.
The revision surgery for cementless implants is much easier due to the availability of good bone stock. Although there are fewer problems of cementless fixation they have in use only recently. The long term advantages and drawbacks are yet not fully understood.
With the advancement in implant materials, there is a growing interest in the cementless fixation of knee implants. Hybrid fixations have also been done where the femoral component is fixed cementless and the tibia is fixed with bone cement.
Comparing the Two Methods
When deciding between cemented and cementless knee replacement, several factors come into play. Cemented knee replacements offer immediate stability and have a long track record of success. However, there is a small risk of cement-related complications, such as allergic reactions or bone cement implantation syndrome. On the other hand, cementless knee replacements provide a more biologic fixation and may be preferred for younger patients or those with good bone quality. However, they may require a longer recovery period as the bone needs time to grow into the implant surfaces.
Factors to Consider: When discussing knee replacement options with your orthopedic surgeon, several factors should be taken into consideration:
Age and Activity Level: Younger, more active patients may benefit from cementless knee replacements, as they provide excellent long-term stability and durability.
Bone Quality: Patients with poor bone quality may be better suited for cemented knee replacements, as the cement provides immediate fixation and stability.
Surgical Technique: The surgeon’s experience and preference may also play a role in determining the best approach for your knee replacement surgery.
Long-Term Success Rates: Both cemented and cementless knee replacements have been shown to have good long-term success rates, but individual outcomes may vary.
Recovery and What to Expect After Treatment
Recovery from knee replacement surgery involves:
- Physical Therapy: Focuses on improving flexibility, strength, and function. The rehabilitation process typically takes several months, with most patients resuming daily activities within 3-6 months.
- Pain Management: Post-surgical pain is typically managed with medications, and swelling is reduced with ice and elevation.
- Lifestyle Adjustments: Patients are encouraged to maintain a healthy weight and engage in low-impact activities to prevent additional stress on the knee joint.
Possible Risks or Side Effects (Complications)
As with any surgery, knee replacement carries risks, including:
- Infection: Post-surgical infections can lead to complications and require further treatment.
- Blood Clots: Deep vein thrombosis (DVT) can occur, requiring blood thinners.
- Implant Loosening: Over time, implants may loosen, requiring revision surgery, particularly with cemented prostheses.
- Nerve or Blood Vessel Damage: These are rare but can occur during surgery.
Long-Term Outlook (Prognosis)
Total knee replacement surgery has a high success rate, with most patients experiencing significant pain relief and improved function. The lifespan of the prosthetic components is typically 15-20 years for cemented prostheses, and the longevity of cementless prostheses may improve over time as bone growth into the implant provides long-term fixation. Both types of implants have shown good long-term success rates, though individual outcomes may vary based on factors like age, activity level, and bone quality.
Insurance & Cost
We work with Medicare, most commercial insurance carriers (Aetna, Anthem BCBS, Cigna, Empire BCBS, UnitedHealthcare), and most workers’ compensation and no-fault insurance carriers. Coverage for cemented and cementless knee replacement depends on your specific plan and the medical necessity criteria that apply to your case. Call our billing team at (631) 981-2663 before scheduling to verify your coverage and discuss expected out-of-pocket costs.
For the full list of carriers we accept and patient billing protections, see our Insurance Information page.
Frequently Asked Questions (FAQ)
Q. What is the difference between cemented and cementless knee replacement?
A. Cemented knee replacement uses bone cement to fix the prosthesis in place, while cementless knee replacement relies on the bone growing into the implant’s porous surface for fixation.
Q. Which is better, cemented or cementless knee replacement?
A. Both methods have their advantages. Cemented knee replacement offers immediate stability and is ideal for patients with poor bone quality. Cementless knee replacement may be preferred for younger patients with good bone quality, as it provides biological fixation and may have longer-term durability.
Q. How long does a knee replacement last?
A. Knee replacements typically last 15-20 years, though the longevity of the implant can vary depending on factors such as the patient’s age, activity level, and bone quality.
Q. How long is the recovery after knee replacement surgery?
A. Recovery usually takes several months, with most patients regaining full function within 3-6 months, although rehabilitation is an ongoing process.
Summary and Takeaway
Both cemented and cementless knee replacements are effective surgical options for treating knee arthritis and joint degeneration. Cemented implants provide immediate stability and are often used in older patients or those with poor bone quality, while cementless implants offer biological fixation and may be preferred for younger, more active individuals. Choosing the appropriate technique depends on factors like age, activity level, bone quality, and the surgeon’s expertise.
Clinical Insight & Recent Findings
A recent study compared cemented and cementless total knee replacement (TKA) techniques, analyzing outcomes based on several factors, including revision rates, functional results, and complications.
Cemented TKA remains the gold standard, particularly in elderly and osteoporotic patients, due to its established long-term success. However, cementless TKA, offering biological fixation and potential for better durability, has gained traction, particularly in younger, active patients. The review found that while cementless TKA showed similar survival rates to cemented procedures, it was associated with fewer complications such as infection and loosening in younger patients.
Notably, cementless fixation allows for easier revision procedures due to better bone preservation. However, precise surgical technique is essential, as cementless implants require more accurate bone cuts. (“Study of cemented vs. cementless knee replacement – See PubMed.”)
Who Performs This Treatment? (Specialists and Team Involved)
Orthopedic surgeons specializing in joint replacement surgery perform knee replacement surgeries. Rehabilitation specialists, including physical therapists, play a key role in post-surgical recovery and functional restoration.
When to See a Specialist?
If you experience persistent knee pain, limited mobility, or instability despite non-surgical treatments, it may be time to consult an orthopedic specialist to discuss knee replacement options.
When to Go to the Emergency Room?
Seek emergency care if you experience severe knee pain, swelling, or signs of infection after surgery, such as increased redness, warmth, or fever.
What Recovery Really Looks Like?
Recovery from knee replacement surgery involves a structured rehabilitation program, with physical therapy to restore strength and flexibility. Full recovery can take several months, with gradual return to normal activities.
What Happens If You Ignore It?
Ignoring knee arthritis or joint degeneration can lead to worsening pain, joint deformity, and reduced mobility. Timely intervention with knee replacement surgery can alleviate symptoms and improve function.
How to Prevent It?
Maintaining a healthy weight, avoiding excessive strain on the knee, and engaging in low-impact exercises can help protect the knee joint and reduce the risk of arthritis and cartilage damage.
Nutrition and Bone or Joint Health
A diet rich in calcium, vitamin D, and omega-3 fatty acids can support joint health and reduce the risk of cartilage damage.
Activity and Lifestyle Modifications
Low-impact activities like swimming and cycling can help maintain joint function without putting excessive strain on the knee. Regular strengthening exercises can also help protect the knee joint and improve stability.
Do you have more questions?
What are the main differences between cemented and cementless knee replacements?
The main difference lies in how the artificial components are secured to the existing bone. Cemented knee replacements use bone cement for immediate fixation, while cementless knee replacements rely on bone ingrowth for biological bonding over time.
Is one method generally preferred over the other?
There isn’t a one-size-fits-all answer. The choice between cemented and cementless knee replacements depends on factors like patient age, bone quality, and surgeon preference.
Are there any specific risks associated with cemented knee replacements?
While cemented knee replacements have been used successfully for many years, there is a small risk of complications related to the bone cement, such as allergic reactions or bone cement implantation syndrome.
What are the benefits of cementless knee replacements?
Cementless knee replacements offer a more biologic fixation, which can be advantageous for younger, more active patients. They also eliminate the risk of complications related to bone cement.
How long does it take for bone to grow into the porous surfaces of cementless knee replacements?
Bone ingrowth typically occurs over several months to a year after surgery, gradually providing stability and durability to the implant.
Are cementless knee replacements suitable for all patients?
While cementless knee replacements can provide excellent long-term stability, they may not be suitable for patients with poor bone quality or certain medical conditions.
Do cemented knee replacements have a higher risk of loosening over time?
While loosening can occur with any type of knee replacement, cemented knee replacements have a proven track record of long-term success and stability for many patients.
How do surgeons determine which type of knee replacement is best for a particular patient?
Surgeons consider factors such as patient age, activity level, bone quality, and their own experience and preference when determining the most appropriate approach for knee replacement surgery.
Can a patient switch from one type of knee replacement to another if needed?
While it’s technically possible to revise a knee replacement from cemented to cementless or vice versa, it’s a more complex procedure with its own set of risks and considerations.
Are there any lifestyle changes or precautions needed after knee replacement surgery?
Patients typically undergo physical therapy and rehabilitation to regain strength and range of motion in the knee. They may also need to avoid certain high-impact activities to prolong the life of the implant.
What is the typical recovery time after knee replacement surgery?
Recovery time can vary depending on factors like surgical approach, patient age, and overall health. Generally, patients can expect to resume light activities within a few weeks and gradually increase activity levels over several months.
How common are complications with knee replacement surgery?
While knee replacement surgery is generally safe, there are risks of complications such as infection, blood clots, and nerve damage. However, these risks are relatively low and can be minimized with proper pre-operative evaluation and surgical technique.
Can knee replacements wear out over time?
While knee replacements can experience wear and tear over time, modern implants are designed to withstand the demands of daily activity for many years. Regular follow-up appointments with the orthopedic surgeon can help monitor the condition of the implant.
How soon can patients expect to return to normal activities after knee replacement surgery?
Recovery times can vary, but most patients can expect to return to light activities within a few weeks and gradually increase activity levels over several months. Full recovery may take several months to a year.
Are there any limitations on physical activity after knee replacement surgery?
While patients can typically resume low-impact activities like walking, swimming, and cycling after knee replacement surgery, they may need to avoid high-impact
What should patients expect during the initial consultation with an orthopedic surgeon for knee replacement surgery?
During the initial consultation, the orthopedic surgeon will evaluate the patient’s medical history, perform a physical examination, and discuss treatment options, including the risks and benefits of knee replacement surgery.
How can patients prepare for knee replacement surgery?
Preparing for knee replacement surgery may include lifestyle modifications, such as quitting smoking or losing weight, as well as arranging for assistance with daily tasks during the recovery period. The orthopedic surgeon will provide specific pre-operative instructions based on the patient’s individual needs.
The content on this page has been authored, edited, or approved by the doctors below, and was last reviewed for accuracy on May 16, 2026.

