Minimally invasive and total knee replacement are two surgical options used to treat severe knee arthritis. Both procedures replace the damaged parts of the knee with artificial implants to reduce pain and improve movement. The difference lies in how much tissue is moved during surgery. Minimally invasive surgery uses a smaller incision and less tissue cutting, while the traditional total knee replacement uses a larger incision for better visibility. Both techniques aim to restore knee function and improve quality of life.
How Common It Is and Who Gets It? (Epidemiology)
Knee replacement is a common surgery performed on many adults each year. It is most often recommended for people with advanced arthritis that causes ongoing pain and stiffness. Both minimally invasive and traditional total knee replacement are used in adults of many ages, especially those whose pain limits daily activities.
Why It Happens – Causes (Etiology and Pathophysiology)
Knee arthritis occurs when the smooth surface of the knee wears down over time. This leads to pain, swelling, stiffness, and difficulty walking. When these symptoms become severe and non-surgical treatments no longer help, knee replacement is considered. The goal is to remove the worn surfaces and replace them with artificial parts that allow smoother movement.
How the Body Part Normally Works? (Relevant Anatomy)
The knee joint is formed by the thigh bone, the shin bone, and the kneecap. Healthy cartilage allows these bones to glide smoothly. The quadriceps tendon and patellar tendon help straighten the leg. When arthritis damages the joint, movement becomes painful and difficult. Knee replacement restores the contact surface so the joint can bend and straighten more easily.
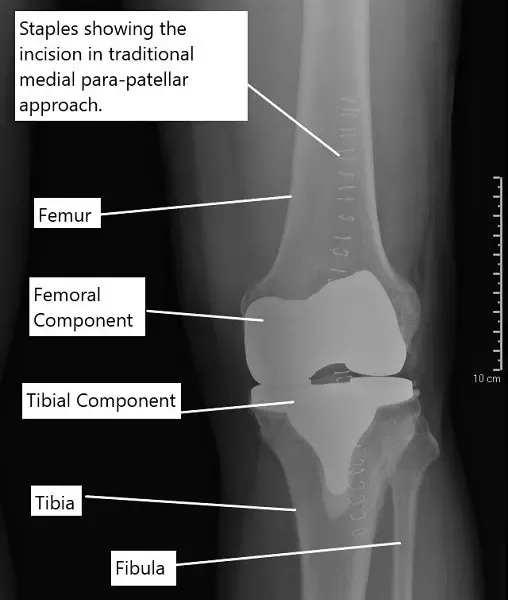
X-ray showing the staples over the incision of a traditional knee replacement done.
What You Might Feel – Symptoms (Clinical Presentation)
People with severe knee arthritis often feel pain, swelling, stiffness, grinding, and trouble walking or climbing stairs. The knee may feel unstable or weak. Some people notice changes in the shape of their leg, such as bowing inward or outward.
How Doctors Find the Problem? (Diagnosis and Imaging)
Diagnosis is based on your symptoms, a physical exam, and imaging tests. X-rays show the amount of cartilage loss and whether the bones are rubbing together. Doctors use this information to decide whether surgery is needed and which type may be best.
Classification
Knee arthritis may be described as mild, moderate, or severe. Minimally invasive knee replacement is usually recommended for patients without severe deformity and with good tissue quality. Traditional knee replacement is used in all cases and may be preferred in patients with more complex knee issues.
Other Problems That Can Feel Similar (Differential Diagnosis)
Conditions that may feel similar to severe knee arthritis include meniscus tears, tendon irritation, bursitis, ligament injuries, and referred pain from the hip or lower back. A detailed exam and imaging help separate these problems from arthritis that requires surgery.
Treatment Options
Non-Surgical Care
Before considering surgery, patients may try rest, activity changes, physical therapy, braces, weight control, and anti-inflammatory medicines. Injections may also help temporarily.
Surgical Care
Traditional total knee replacement uses a larger incision and allows the surgeon to see the entire joint clearly. The quadriceps tendon is partially opened, and the kneecap is moved aside. The worn bone surfaces are shaped to fit the artificial implants, which are secured with bone cement.
Minimally invasive knee replacement uses a smaller incision and less tissue cutting. The surgeon lifts part of the inner thigh muscle instead of cutting the quadriceps tendon. Implants are similar to those used in the traditional method. This technique can reduce early pain, lessen blood loss, and allow earlier movement, but it is not suitable for all patients.
Traditional knee replacement surgery
During a traditional knee replacement surgery, the surgeon gives an incision in front of the knee joint. After dissecting the tissues, the surgeon cuts the quadriceps tendon along the side of the kneecap. A tissue along the side of the patellar tendon (an extension of the quadriceps tendon) is also cut.
The quadriceps tendon attached to the four quadriceps muscles present in front of the thigh. The four quadriceps muscles help in the extension of the leg at the knee joint. The integrity of the muscles, quadriceps tendon, patella, knee joint, and patellar tendon is required for straightening the leg.
The kneecap is then usually everted to get a better exposure of the joint. The surgeon then proceeds to surgically cut the bone ends of the thigh bone and the shin bone. The cuts are made to contour the shape so the prosthetic implants fit over the cut ends.
While the bony preparation of the cut ends is an important aspect of the replacement surgery, the most crucial part in stabilizing the knee joint. Stabilizing the artificial joint requires balancing the forces acting around the knee joint. The diseased knee joint is often deformed (knock knees or bow legs). The deformity is also corrected during the surgery.
After the knee is balanced, metal prosthetic parts are fixed using bone cement on the thigh bone and the shin bone. A high-grade plastic is inserted in between the metal parts to smoothen the motion. The incision is closed in layered and the patient is usually able to walk the evening of the surgery or the next day.
Minimally invasive knee replacement
Minimally invasive knee replacement technique involves a smaller incision and less cutting of the tissue. The surgeon gives a smaller incision and instead of cutting the quadriceps tendon, the surgeon lifts the vastus medialis muscle. In some techniques, the vastus medialis may be cut instead of the quadriceps tendon.
The surgeon then accesses the knee joint similarly but may not dislocate the tibia to perform the bone cuts. Implants similar to a traditional knee replacement are fixed using bone cement. The incision is then closed in layers. Some advantages of a minimally invasive technique are:
- A small skin incision leads to a smaller scar on the knee which may be aesthetically important for some patients.
- A small incision and less cutting of the tissues leads to less intraoperative blood loss as compared to the traditional approach.
- Patients treated with minimally invasive techniques are able to start the rehabilitation process earlier and may have to stay at the hospital for fewer days as compared to traditional. Although, recent studies have suggested similar postoperative stays for both traditional and minimally invasive.
- As less tissue is cut during a minimally invasive technique, the patients may be expected to experience less postoperative pain.
However, there may be potential disadvantages to a minimally invasive knee replacement surgery.
- The surgeon works with a very small field of surgery using a minimally invasive technique. The small field of surgery may potentially interfere with the correct placement of the implants.
- The narrow field of surgery may also lead to potential stretching of the tissues while using the retractors. The stretching may also lead to rupture of the patellar tendon.
- The minimally invasive technique may not be used in all patients. The technique is generally not indicated in patients who are obese, muscular, or with severe deformities such as bow legs or knock knees.
- The technique also has a difficult learning curve for the surgeon as compared to the traditional approach.
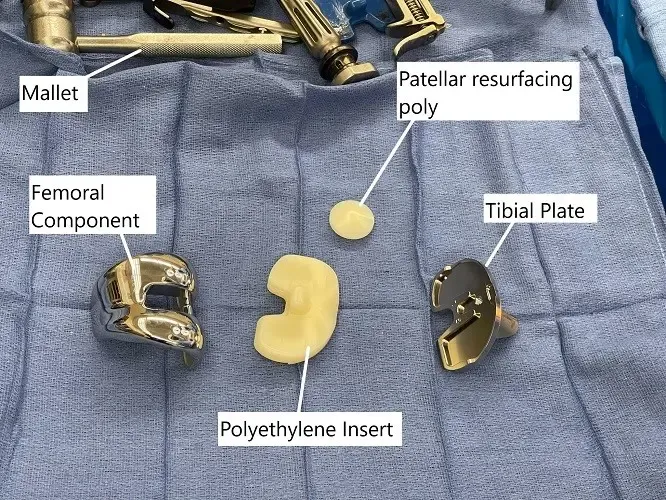
Intraoperative image showing the implants used in a total knee replacement surgery.
Recent studies have indicated similar outcomes in both the traditional approach and the minimally invasive approach. As discussed earlier, a knee replacement surgery is much more than simply replacing the ends of the bone. The long-term survival of the implants depends a great deal upon the intraoperative balancing of the knee and the stability of the joint in motion.
Knee replacement surgeries have revolutionized the management of knee pain due to arthritis. A vast number of patients benefit from knee replacement surgeries annually. The traditional approach has been in use for many years and has excellent results.
While the minimally invasive approach has a number of potential benefits, the technique may not be suitable for all patients and requires greater surgical expertise. Speak with your orthopedic surgeon, what type of knee replacement technique may be best suited in your case.
Recovery and What to Expect After Treatment
Recovery includes several weeks of physical therapy to improve movement and build strength. Many patients begin walking the day of surgery or the next day. Minimally invasive surgery may allow quicker early recovery, but long-term results are similar for both methods. Following the rehabilitation plan is one of the most important parts of healing.
Possible Risks or Side Effects (Complications)
Risks include infection, blood loss, stiffness, and implant positioning problems. With minimally invasive surgery, the smaller working area can make implant placement more difficult and may increase the chance of tendon stretching. Not all patients are good candidates for minimally invasive surgery, especially those who are muscular, obese, or have severe deformity.
Long-Term Outlook (Prognosis)
Studies show that both minimally invasive and traditional knee replacement have similar long-term results. Implants last for many years, and most patients experience major improvement in pain and daily activity. The success of the surgery depends on proper knee balancing during the procedure and strong rehabilitation afterward.
For insurance and cost information, see our Insurance Information page.
Frequently Asked Questions (FAQ)
Q. Which surgery heals faster?
A. Minimally invasive surgery may lead to quicker early recovery, but long-term results are similar.
Q. Is minimally invasive knee replacement better?
A. It offers benefits for some patients, but not everyone is a candidate.
Q. Will I walk the same day?
A. Many patients walk the same day or the next day after either procedure.
Q. Does minimally invasive surgery hurt less?
A. It may reduce early discomfort because less tissue is cut.
Q. How long do implants last?
A. Most implants last many years, but this depends on activity level and overall health.
Summary and Takeaway
Minimally invasive and traditional total knee replacement both aim to relieve pain and restore movement in people with advanced arthritis. The minimally invasive technique uses a smaller incision and less tissue cutting, which may reduce early pain and speed up initial recovery. Traditional surgery offers excellent visibility and is suitable for all patients. Long-term results for both techniques are similar, and the best option depends on your knee condition and overall health.
Clinical Insight & Recent Findings
A recent study comparing total knee replacement with a less invasive combined procedure—unicompartmental knee replacement performed alongside anterior cruciate ligament reconstruction—found that long-term pain relief, function, and radiographic outcomes were essentially the same between groups, with no increase in complications for the less invasive approach .
These findings support the broader points outlined above: while minimally invasive knee replacement techniques can offer smaller incisions, reduced blood loss, and earlier rehabilitation, long-term results often mirror those of traditional total knee replacement, which remains reliable and effective for many patients.
The study reinforces that patient selection and precise surgical technique are more important than incision size alone, echoing the text’s emphasis that implant positioning, joint balancing, and correction of deformity ultimately determine durability and outcomes. (“Study of knee replacement techniques – see PubMed.”)
Who Performs This Treatment? (Specialists and Team Involved)
Orthopedic surgeons perform both types of knee replacement. They work with physician assistants, nurses, and physical therapists who guide care before and after surgery.
When to See a Specialist?
You should see a knee specialist if knee pain interferes with daily life, keeps returning, or does not improve with non-surgical treatments. A specialist can help determine whether surgery is needed and which technique fits your situation.
When to Go to the Emergency Room?
Seek emergency care if the knee becomes suddenly swollen, very painful, or unable to bear weight. A high fever, redness, or drainage after surgery also requires immediate attention.
What Recovery Really Looks Like?
Recovery involves guided exercises, walking with support, and slow improvement in strength and flexibility. Some people feel better quickly, while others take longer depending on their health and the amount of arthritis they had before surgery.
What Happens If You Ignore It?
Ignoring severe knee arthritis can lead to increased pain, more stiffness, and difficulty walking. The joint may continue to wear down, making daily activities harder and limiting treatment options.
How to Prevent It?
Maintaining a healthy weight, staying active, building leg strength, and avoiding high-impact activities can help reduce stress on the knee. Early care for knee injuries may also prevent later problems.
Nutrition and Bone or Joint Health
Eating foods that support bone and joint health—such as those rich in vitamin D, calcium, and protein—can help support recovery. Staying hydrated helps keep the joints functioning well.
Activity and Lifestyle Modifications
Low-impact activities such as walking, cycling, and swimming help maintain knee strength after surgery. Avoiding twisting movements, heavy lifting, and high-impact sports protects the joint and helps the implants last longer.
Do you have more questions?
What are the long-term outcomes like for minimally invasive knee replacement?
Long-term outcomes can be similar to traditional knee replacement, especially if the surgery is performed by an experienced surgeon. The key factors are accurate placement of the prosthesis and the patient’s adherence to rehabilitation.
Will I need physical therapy after surgery?
Yes, physical therapy is crucial for recovery and to achieve the best possible function of the knee.
Are there any weight restrictions for minimally invasive knee replacement?
Yes, patients who are significantly overweight may not be ideal candidates for minimally invasive surgery due to the stress on the smaller implants and technical difficulties in surgery.
What is the expected lifespan of knee implants from either surgery?
Knee implants generally last 15-20 years, but longevity can vary based on activity levels, weight, and other health factors.
Are there activities I should avoid after knee replacement?
High-impact activities like running, jumping, or contact sports are generally discouraged to prolong the life of the implant.
What happens if the knee replacement fails?
If the implant fails or wears out, a revision surgery might be necessary. This is more complex and involves replacing the old implants with new ones.
How soon can I drive after surgery?
Patients can usually drive 4 to 6 weeks after surgery, once they have sufficient pain control and can operate the vehicle safely.
What are the signs of infection to watch out for after surgery?
Signs include excessive swelling, redness, pain, fever, and drainage from the incision site. Immediate medical consultation is necessary if these occur.
Can minimally invasive surgery be done on both knees at the same time?
It is technically possible but not commonly recommended due to the increased risk and recovery complexity.
What are the financial considerations for these types of surgeries?
Costs can vary significantly based on location, hospital, insurance coverage, and the specific needs of the patient. It’s important to discuss these with your healthcare provider and insurance company.
How do I know if my insurance will cover these surgeries?
Check with your insurance provider for details about coverage for knee replacement surgery, which typically is covered when medically necessary.
What are common complications with knee replacements?
Complications can include infection, blood clots, implant loosening, or wear. Prompt medical attention can manage these issues if they occur.
How effective is minimally invasive knee replacement compared to traditional knee replacement?
Both methods are effective for relieving pain and improving function. The choice of technique mainly affects the recovery process and immediate post-operative pain.
What should I look for in a surgeon if considering a minimally invasive knee replacement?
Look for a surgeon who is specially trained in minimally invasive techniques and has a track record of successful outcomes. Surgeon experience is critical to minimize risks associated with the limited visibility of the surgery site.
How do I manage pain after knee replacement surgery?
Pain management includes medications, ice, elevation, and guided physical therapy. Advanced pain management techniques like nerve blocks are also used.
What improvements can I expect in my knee function after surgery?
Most patients experience significant improvement in pain and mobility. The goal is to return to everyday activities without the pain that was present before surgery.
How soon after knee replacement surgery can complications typically arise?
Complications after knee replacement surgery can arise at various times during the postoperative period, ranging from the immediate postoperative period to months or even years after surgery. It’s essential to remain vigilant for signs and symptoms of complications and seek prompt medical attention if any concerns arise.
Are there any specific precautions or considerations for patients with certain medical conditions (e.g., diabetes, heart disease) undergoing knee replacement surgery?
Patients with medical conditions may require additional preoperative evaluation and optimization to reduce the risk of complications during and after knee replacement surgery. Close coordination between the orthopedic surgeon and other medical specialists is essential to ensure safe and successful outcomes.
Are there any emerging technologies or advancements in knee replacement surgery that patients should be aware of?
Emerging technologies such as patient-specific implants, 3D printing, and advanced surgical navigation systems are being explored to further improve the precision and outcomes of knee replacement surgery.
How long does it typically take to recover from knee replacement surgery, and what is the rehabilitation process like?
Recovery time can vary, but most patients undergo several weeks of physical therapy to regain strength, mobility, and function in the replaced knee.
What factors determine the success rate of knee replacement surgery, and how can patients optimize their outcomes?
Success rates depend on factors such as patient age, overall health, severity of knee damage, surgical technique, implant selection, and adherence to post-operative rehabilitation protocols.
Are there alternatives to traditional knee replacement surgery, such as partial knee replacement or minimally invasive procedures?
Yes, alternatives include partial knee replacement for localized knee arthritis and minimally invasive techniques that aim to preserve more healthy tissue and facilitate quicker recovery.
The content on this page has been authored, edited, or approved by the doctors below, and was last reviewed for accuracy on May 17, 2026.

