Minimally invasive and traditional total knee replacement are two ways to do the same operation: replacing the worn parts of an arthritic knee with artificial parts to ease pain and restore movement.
The difference is how much tissue is disturbed to get to the joint. The minimally invasive approach uses a smaller incision and less cutting, while the traditional approach uses a larger incision for a clearer view. Long-term results are similar, and the right choice depends on your knee and your overall health.
About knee arthritis
The knee is formed by the thigh bone, shin bone, and kneecap, with smooth cartilage letting the bones glide and the quadriceps and patellar tendons straightening the leg. In arthritis, that smooth surface wears down over time, so the bones rub and the joint becomes painful, swollen, and stiff.
When the wear is severe and non-surgical care no longer helps, a knee replacement removes the worn surfaces and replaces them with artificial parts that move more smoothly.
Symptoms
People with advanced knee arthritis often have pain, swelling, stiffness, grinding, and trouble walking or climbing stairs. The knee can feel weak or unstable, and some people notice their leg changing shape, bowing inward or outward.
How it is diagnosed
Diagnosis is based on your symptoms, a physical exam, and X-rays, which show how much cartilage is lost and whether the bones are rubbing together.
This also helps the surgeon decide whether surgery is needed and which technique fits. Other problems can feel similar, including meniscus tears, tendon irritation, bursitis, ligament injuries, and pain referred from the hip or lower back, so a careful exam matters.
When to consider knee replacement
Surgery is not the first step. Most people first try rest, activity changes, physical therapy, braces, weight control, anti-inflammatory medicines, and sometimes injections, which can help for a while.
A replacement is considered when arthritis is severe, the pain limits daily life, and these measures no longer give enough relief.
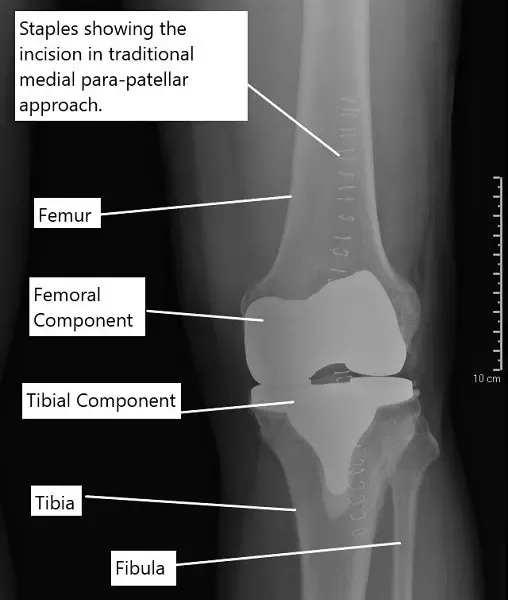
X-ray showing the staples over the incision of a traditional knee replacement done.
Traditional total knee replacement
In the traditional approach, the surgeon makes a larger incision at the front of the knee for a clear view of the whole joint. The quadriceps tendon is partly opened along the side of the kneecap, and the kneecap is moved aside (and often flipped) to expose the joint.
The worn ends of the thigh bone and shin bone are then cut and shaped so the artificial parts fit. A key part of the operation is balancing the knee and correcting any deformity (such as bowlegs or knock knees), because that stability is what makes the new joint last.
The metal parts are fixed with bone cement, a durable plastic spacer goes between them, and the incision is closed in layers. Many people walk the evening of surgery or the next day.
Minimally invasive knee replacement
The minimally invasive approach uses a smaller incision and disturbs less tissue. Instead of cutting the quadriceps tendon, the surgeon lifts the inner thigh muscle (the vastus medialis) to reach the joint. The implants are the same as in the traditional method and are fixed with bone cement. Reported advantages include:
- A smaller scar
- Less blood loss during surgery, because less tissue is cut.
- Earlier rehab and sometimes a shorter hospital stay, though recent studies show stays are often similar to the traditional approach.
- Possibly less pain early on, since less tissue is disturbed.
Trade-offs of the minimally invasive approach
The smaller incision comes with real limitations, which is why it is not used for everyone:
- The surgeon works through a small window, which can make placing the implants accurately more difficult.
- Pulling on the tissues with retractors can stretch them, and in some cases this can tear the patellar tendon.
- It is generally not suitable for people who are overweight, very muscular, or who have severe deformities like bowlegs or knock knees.
- It is technically harder and has a steeper learning curve for the surgeon.
How the two compare
Recent studies show similar long-term results for both approaches. That is because a knee replacement is much more than trimming the bone ends.
The long-term survival of the implant depends heavily on balancing the knee during surgery and getting the joint stable through its full range of motion, not on the size of the incision.
The traditional approach has been used for many years with reliable results and works for every patient. The minimally invasive approach has appealing short-term benefits, but it is not right for everyone and demands more surgical experience.
The best choice is one to make with your surgeon based on your knee and your health.
Recovery
Recovery for both involves several weeks of physical therapy to rebuild movement and strength, and many people start walking the day of surgery or the next day.
The minimally invasive approach may give a quicker early recovery, but the long-term results are similar. Following the rehab plan closely is one of the most important parts of healing.
Risks
Both operations carry the general risks of surgery, including infection, blood loss, stiffness, and problems with implant positioning. With the minimally invasive approach, the smaller working area can make implant placement harder and raises the chance of stretching or tearing a tendon.
Not everyone is a candidate, particularly people who are muscular, overweight, or have a severe deformity.
Protecting your knee long-term
After surgery, low-impact activities like walking, cycling, and swimming help keep the knee strong and flexible. Keeping a healthy weight, building leg strength, and avoiding twisting, heavy lifting, and high-impact sports all take stress off the joint and help the implants last longer.
When to see a doctor
See a knee specialist if knee pain interferes with daily life, keeps returning, or does not improve with non-surgical care. Seek emergency care if the knee becomes suddenly swollen, very painful, or unable to bear weight, or if you have a high fever, redness, or drainage after surgery.
How Medicare Covers Total Knee Replacement Implants
If you have Medicare, your healthcare provider may bill for CPT Code 27447. This is a surgical procedure where the damaged knee joint is removed and replaced with an artificial knee.
What is the out-of-pocket cost:
Estimated Out-of-Pocket Cost for Total Knee Replacement Implants (27447): $259.73
Medicare approves about $1,298.63 for this procedure and pays 80% of it ($1,038.90). The remaining 20% is the patient’s responsibility.
“For example, hypothetical patient, Stacy, needed a total knee replacement. Her procedure was a replacement of her knee joint with an artificial implant (27447). Thanks to Medicare, her total out-of-pocket cost was about $259.73. Her secondary insurance then covered it completely!”
For insurance and cost information, see our Insurance Information page.
Do you have more questions?
What is the expected lifespan of knee implants from either surgery?
Knee implants generally last 20+ years, but longevity can vary based on activity levels, weight, and other health factors.
What happens if the knee replacement fails?
If the implant fails or wears out, a revision surgery might be necessary. This is more complex and involves replacing the old implants with new ones.
How soon can I drive after surgery?
Patients can usually drive 4 to 6 weeks after surgery, once they have sufficient pain control and can operate the vehicle safely.
What are the signs of infection to watch out for after surgery?
Signs include excessive swelling, redness, pain, fever, and drainage from the incision site. Immediate medical consultation is necessary if these occur.
Can minimally invasive surgery be done on both knees at the same time?
It is technically possible but not commonly recommended due to the increased complication risks and recovery complexity.
What are the financial considerations for these types of surgeries?
Costs can vary significantly based on location, hospital, insurance coverage, and the specific needs of the patient. It’s important to discuss these with your healthcare provider and insurance company.
How do I know if my insurance will cover these surgeries?
Check with your insurance provider for details about coverage for knee replacement surgery, which typically is covered when medically necessary.
What are common complications with knee replacements?
Complications can include infection, blood clots, implant loosening, or wear. Prompt medical attention can manage these issues if they occur.
What should I look for in a surgeon if considering a minimally invasive knee replacement?
Look for a surgeon who is specially trained in minimally invasive techniques and has a track record of successful outcomes. Surgeon experience is critical to minimize risks associated with the limited visibility of the surgery site.
How do I manage pain after knee replacement surgery?
Pain management includes medications, ice, elevation, and guided physical therapy. Advanced pain management techniques like nerve blocks are also used.
What improvements can I expect in my knee function after surgery?
Most patients experience significant improvement in pain and mobility. The goal is to return to everyday activities without the pain that was present before surgery.
How soon after knee replacement surgery can complications typically arise?
Complications after knee replacement surgery can arise at various times during the postoperative period, ranging from the immediate postoperative period to months or even years after surgery. It’s essential to remain vigilant for signs and symptoms of complications and seek prompt medical attention if any concerns arise.
What factors determine the success rate of knee replacement surgery, and how can patients optimize their outcomes?
Success rates depend on factors such as patient age, overall health, severity of knee damage, surgical technique, implant selection, and adherence to post-operative rehabilitation protocols.
Are there alternatives to traditional knee replacement surgery, such as partial knee replacement or minimally invasive procedures?
Yes, alternatives include partial knee replacement for localized knee arthritis and minimally invasive techniques that aim to preserve more healthy tissue and facilitate quicker recovery.
The content on this page has been authored, edited, or approved by the doctors below, and was last reviewed for accuracy on July 2, 2026.

