Natural History of Odontoid Fracture
If neck pain becomes severe enough to disrupt daily activities or is accompanied by swelling, tenderness, or redness, it is important to seek medical attention.
At Complete Orthopedics, our skilled spine specialists excel in treating cervical spine and neck pain using both surgical and non-surgical methods. We evaluate symptoms, identify the problem, and suggest suitable treatments, including surgery if necessary.
We serve the New York City and Long Island areas, partnering with six hospitals to offer cutting-edge cervical spine surgery and comprehensive orthopedic care. You can book an appointment with our orthopedic surgeons online or by phone.
Learn about common causes of neck pain and the treatment options available, including when surgery might be the best choice.
Overview
Cervical spine fractures, particularly those involving the C2 vertebra or odontoid process, are significant injuries. The odontoid, a bony projection of the C2 vertebra, plays a crucial role in stabilizing the neck and enabling head movements. Injuries to this area can be severe, and understanding them is key to effective treatment and recovery.
Prevalence and Causes
Odontoid fractures account for up to 20% of cervical spine fracture cases. These injuries are common in two main groups: older adults and younger adults, each with different primary causes.
Older Adults:
-
- Cause: Falls from a standing height.
- Reason: As people age, bones become more fragile, making them more susceptible to fractures from relatively minor falls.
Younger Adults:
-
- Cause: High-energy traumas such as motor vehicle accidents (MVAs) or significant falls.
- Reason: High-impact incidents exert substantial force on the spine, leading to fractures. These cases often involve additional injuries to the head, face, and lower cervical spine.
In motor vehicle accidents, particularly those involving frontal impacts, the force exerted on the head and neck often results in odontoid fractures.
Types of Odontoid Fractures
The classification of odontoid fractures is essential for determining the appropriate treatment. The most commonly used classification system was developed by Anderson and D’Alonzo in 1974 and includes three types:
Type I:
-
- Description: An oblique fracture at the upper part of the odontoid process.
- Implication: Often considered stable but requires careful monitoring.
Type II:
-
- Description: A fracture at the junction between the odontoid process and the vertebral body.
- Implication: The most common type and often unstable, posing a significant risk for nonunion (failure to heal properly).
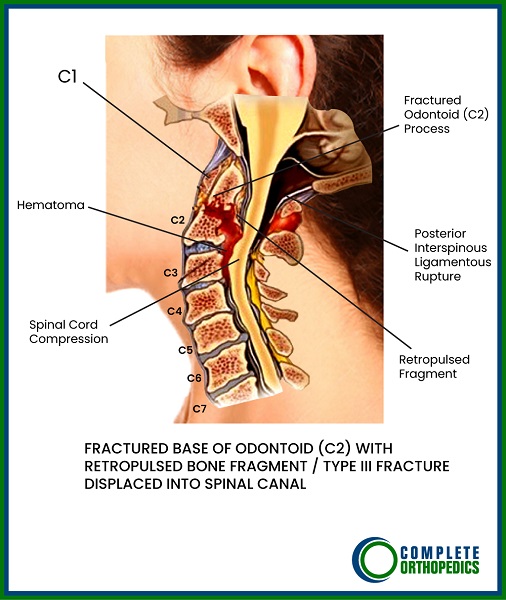
Type III:
-
- Description: A fracture that extends into the C2 vertebral body.
- Implication: Generally more stable than Type II and has a better healing potential due to the larger surface area for bone healing.
Recently, a modified classification scheme by Grauer et al. has been introduced to better distinguish between Type II and Type III fractures and provide more detailed sub-classifications for Type II fractures based on factors like fracture orientation, displacement, and comminution (splintering).
Biomechanics and Injury Mechanisms
Understanding the biomechanics of odontoid fractures helps in grasping why these injuries occur and how they can be prevented. Studies have shown that a mix of horizontal shear and vertical compression forces is necessary to produce the three types of fractures.
- Horizontal Shear: Forces that move the head and neck horizontally.
- Vertical Compression: Forces that compress the head and neck downward.
Sagittal Impacts: The primary cause of odontoid fractures is often a sagittal impact to the head, such as hitting the head on the steering wheel during a car crash.
Experimental Findings:
- Althoff (1979): Demonstrated the necessity of combined shear and compression loading to consistently produce odontoid fractures.
- Mouradian et al.: Successfully induced Type II fractures using a simplified model.
- Nightingale et al.: Observed Type III fractures in the majority of specimens through extension loading (backward bending of the head).
Clinical Observations and Statistics
Clinical studies corroborate the findings of biomechanical research. Data from large patient cohorts highlight the prevalence and causes of odontoid fractures:
Younger Adults:
-
- Leading Cause: Motor vehicle accidents (MVAs).
- Statistics: In a study of 340 patients with axis fractures, 71% were due to MVAs, followed by falls (14%) and diving accidents (4%).
- Type of Injuries: Odontoid fractures were the most common, accounting for 58% of the cases.
Older Adults:
-
- Leading Cause: Falls from standing height.
- Injury Mechanism: Weakened bone and increased loads on the upper cervical spine contribute to the higher frequency of these fractures.
Future Research: Larger sample sizes and younger specimens are necessary to validate these findings further and explore the relationship between cervical spine conditions (e.g., spondylosis, bone mineral density) and odontoid fractures.
Treatment Approaches
Treating odontoid fractures, especially Type II fractures, remains a topic of clinical debate. The goal is to ensure stability, allow proper healing, and restore natural motion.
Conservative Treatments:
-
- Cervical Collar or Halo Vest: Used to immobilize the neck and promote healing. These are non-invasive and often used for less severe or stable fractures.
- Indication: Often suitable for older adults or those with comorbidities that make surgery risky.
Surgical Treatments:
-
- Anterior Odontoid Screw Fixation: This technique involves placing screws through the mouth into the odontoid process to stabilize the fracture. It aims to provide immediate stability while preserving neck motion.
- Posterior Fusion: Involves fusing the C1 and C2 vertebrae to prevent movement and allow the bone to heal. This method is often used for more complex or unstable fractures.
- Indication: Preferred for younger patients, high-energy trauma cases, or when conservative treatment fails.
Postoperative Care:
- Rehabilitation: Physical therapy to restore neck strength and flexibility.
- Follow-Up: Regular imaging (e.g., X-rays, CT scans) to monitor healing.
Future Directions
Biomechanical research continues to advance our understanding of odontoid fractures. Developing more accurate models to replicate the dynamic loads and accelerations experienced during real-life traumatic events is crucial. This research will inform decisions regarding:
- Ligamentous Instability: Understanding the role of ligaments in stabilizing the fracture.
- Reduction Techniques: Methods to realign the fractured bones.
- Patient Positioning: Optimal positions for promoting healing and reducing complications.
- Stabilization Methods: Evaluating different surgical and non-surgical options for each fracture type.
Conclusion
Odontoid fractures are complex injuries with significant implications for the stability and function of the cervical spine. Understanding the prevalence, causes, classification, and treatment options is essential for effective management. Ongoing research and clinical advancements will continue to improve outcomes for patients with these challenging injuries.
Do you have more questions?
What symptoms indicate an odontoid fracture?
Symptoms of an odontoid fracture may include severe neck pain, difficulty moving the neck, numbness or tingling in the arms or legs, and, in severe cases, difficulty breathing or swallowing.
How is an odontoid fracture diagnosed?
Odontoid fractures are diagnosed through imaging studies such as X-rays, CT scans, and MRI. These tests help to visualize the fracture and assess its severity.
What are the risk factors for developing an odontoid fracture?
Risk factors include advanced age, osteoporosis, high-energy trauma such as motor vehicle accidents, and falls from significant heights.
Can odontoid fractures heal on their own without treatment?
Some stable Type I fractures might heal with conservative treatment, but most odontoid fractures, especially Types II and III, require medical intervention to ensure proper healing and prevent complications.
What conservative treatments are available for odontoid fractures?
Conservative treatments include cervical collars or halo vests, which immobilize the neck to allow the fracture to heal naturally.
What are the potential complications of an untreated odontoid fracture?
Untreated odontoid fractures can lead to chronic pain, nonunion (failure to heal), spinal instability, and neurological deficits due to spinal cord compression.
When is surgery necessary for an odontoid fracture?
Surgery is typically necessary for unstable fractures, such as Type II fractures, or when conservative treatment fails to achieve proper alignment and healing.
How long does it take to recover from an odontoid fracture?
Recovery time varies depending on the severity of the fracture and the treatment method. It can range from several weeks to several months.
What are the success rates of surgical treatment for odontoid fractures?
Surgical treatment for odontoid fractures generally has high success rates, with many patients achieving good stability and return to normal activities.
Are there any long-term effects of odontoid fractures?
Long-term effects can include residual neck stiffness, pain, and, in some cases, limited range of motion or neurological deficits if the spinal cord was affected.
Can odontoid fractures be prevented?
Preventing odontoid fractures involves minimizing fall risks, using seat belts and appropriate safety equipment in vehicles, and managing conditions like osteoporosis to strengthen bones.
Are there any specific exercises recommended for patients recovering from odontoid fractures?
Specific exercises should be guided by a physical therapist but generally include gentle range-of-motion exercises, strengthening exercises for the neck and upper back, and postural training.
What lifestyle changes can help in the recovery from an odontoid fracture?
Lifestyle changes that can aid recovery include avoiding high-risk activities, following a healthy diet to support bone healing, and adhering to a structured physical therapy program.
How do odontoid fractures affect daily activities?
Odontoid fractures can significantly impact daily activities due to pain, limited neck movement, and the need for immobilization during healing. Activities requiring neck movement may be particularly challenging.
What is the prognosis for patients with odontoid fractures?
The prognosis for patients with odontoid fractures is generally good, especially with appropriate treatment. Most patients can return to their normal activities, although some may experience lingering symptoms.
What should patients avoid doing while recovering from an odontoid fracture?
Patients should avoid activities that put strain on the neck, such as heavy lifting, sudden head movements, and high-impact sports, until cleared by their healthcare provider.
How does bone density affect the risk of odontoid fractures?
Lower bone density, as seen in conditions like osteoporosis, increases the risk of fractures, including odontoid fractures, due to weaker bones being more susceptible to injury.
How does an anterior odontoid screw fixation work?
An anterior odontoid screw fixation involves inserting a screw through the mouth into the odontoid process to stabilize the fracture. This technique aims to provide immediate stability while preserving neck motion.
What is the role of a halo vest in treating odontoid fractures?
A halo vest is used to immobilize the cervical spine, ensuring proper alignment and stability during the healing process. It is typically used for more severe or unstable fractures.
How do healthcare providers determine the best treatment approach for an odontoid fracture?
The treatment approach is determined based on the type and severity of the fracture, patient age, overall health, and the presence of other injuries or conditions.
What is the role of imaging studies in managing odontoid fractures?
Imaging studies, such as X-rays, CT scans, and MRI, are crucial for diagnosing the fracture, assessing its severity, planning treatment, and monitoring healing progress.
Can patients with odontoid fractures return to sports or physical activities?
Many patients can return to sports or physical activities after recovering from an odontoid fracture, but this should be done gradually and under the guidance of their healthcare provider.
How important is follow-up care after treating an odontoid fracture?
Follow-up care is essential to monitor healing, manage any complications, and adjust treatment plans as needed to ensure the best possible outcome for the patient.

Dr. Vedant Vaksha
I am Vedant Vaksha, Fellowship trained Spine, Sports and Arthroscopic Surgeon at Complete Orthopedics. I take care of patients with ailments of the neck, back, shoulder, knee, elbow and ankle. I personally approve this content and have written most of it myself.
Please take a look at my profile page and don't hesitate to come in and talk.
[et_pb_button admin_label="Button" button_url="https://www.cortho.org/general-appointment/" url_new_window="off" button_text="Schedule an Appointment" button_alignment="center" background_layout="light" custom_button="on" button_text_color="#FFFFFF" button_bg_color="#02770B" button_border_color="#FFFFFF" button_letter_spacing="1" button_font="Arial" button_on_hover="on" button_text_color_hover="#FFFFFF" button_bg_color_hover="#02770B" button_letter_spacing_hover="1" /]