Microscopic and endoscopic discectomy are minimally invasive procedures designed to treat lumbar disc herniation, which often leads to radiculopathy (nerve pain) in the lower back and legs. These techniques have evolved over time, offering significant improvements in surgical precision, recovery time, and patient outcomes compared to traditional open discectomy. The surgery is generally considered when conservative treatments such as medications, physical therapy, and injections have failed to relieve symptoms.
How Common It Is and Who Gets It? (Epidemiology)
Lumbar disc herniation is a common cause of radiculopathy, affecting a significant portion of the active population, especially individuals between 30 and 50 years of age. It is most commonly seen in people who engage in physical activity, heavy lifting, or those with pre-existing degenerative changes in the spine. Approximately 10% of patients with lumbar disc herniation require surgical intervention, such as microdiscectomy or endoscopic discectomy, after conservative treatments fail.
Why It Happens – Causes (Etiology and Pathophysiology)
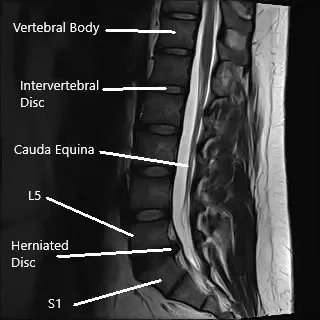
Lumbar disc herniation occurs when the soft inner material of an intervertebral disc (nucleus pulposus) pushes through a tear in the tougher outer layer (annulus fibrosus), placing pressure on nearby spinal nerves. This leads to symptoms such as:
- Radiculopathy: Pain, numbness, tingling, or weakness radiating down the leg, often referred to as sciatica.
- Degenerative Disc Disease: Over time, the discs lose their ability to cushion the vertebrae, making them more susceptible to herniation.
- Trauma or Repetitive Stress: Sudden injury or repetitive movements can increase the risk of disc herniation.
How the Body Part Normally Works? (Relevant Anatomy)
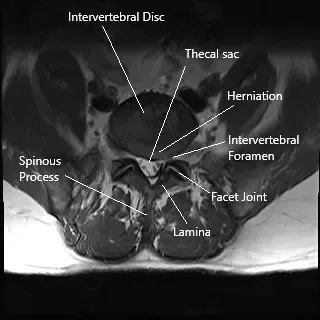
The lumbar spine consists of five vertebrae (L1-L5) with intervertebral discs between them that act as shock absorbers. The spinal cord runs through the spinal canal, and nerves branch out from the cord through small openings called foramina. These nerves transmit signals to various parts of the body, including the legs and feet. When a disc herniates, it can compress these nerves, leading to pain and dysfunction in the lower extremities.
What You Might Feel – Symptoms (Clinical Presentation)
The primary symptoms of lumbar disc herniation that may require surgical intervention include:
- Radicular Pain: Sharp pain radiating down the leg, often following the path of the sciatic nerve.
- Numbness and Tingling: Sensations in the legs or feet, caused by nerve compression.
- Muscle Weakness: Difficulty in walking or performing daily activities due to impaired nerve function.
- Failed Conservative Treatments: Persistent symptoms despite rest, physical therapy, and medications.
How Doctors Find the Problem? (Diagnosis and Imaging)
To diagnose lumbar disc herniation and determine the need for surgery, doctors typically use:
- MRI: The gold standard imaging technique to visualize disc herniation, nerve compression, and other spinal issues.
- CT Scans: Sometimes used when MRI is unavailable or to get more detailed images of the bones.
- X-rays: To rule out other causes of back pain such as fractures or alignment issues.
- Physical Examination: To assess reflexes, strength, and nerve function, often showing signs of radiculopathy.
Classification
Microscopic and endoscopic discectomy can be classified based on the surgical approach:
- Microdiscectomy: Involves using an operating microscope for a small incision to remove the herniated disc material.
- Endoscopic Discectomy: Uses an endoscope (a small camera) for a less invasive approach, often with even smaller incisions.
Technique
After careful selection of the patient for surgery as indicated above, patients are taken to the operating room where they are put under general anesthesia. After anesthesia, the patients are flipped onto their bellies on a special table. All the bony prominences are well padded and the nerves are well padded.
The area of surgery is well-prepped and draped aseptically. X-ray imaging (Fluoroscopy) is used inside the operating room to identify the level before the decision. Once the incision is given, meticulous dissection and hemostasis is achieved and the back of the spine is reached, the level is again checked under x-ray.
For tubular microdiscectomy, a similar approach is performed with the use of sequential dilation and the use of tubes to visualize the area of interest. This requires no muscle stripping and minimal injury to the muscles.
While performing endoscopic discectomy, a camera is used instead of the operating microscope, and the area of surgery is visualized on a monitor. Special instruments are used to the surgery which allows the camera to project as well as perform the surgery.
After confirming the level, some of the bone from the back of the spine is removed to expose the yellow ligament (ligamentum flavum) underneath. The ligament is also excised to expose the nerve roots.
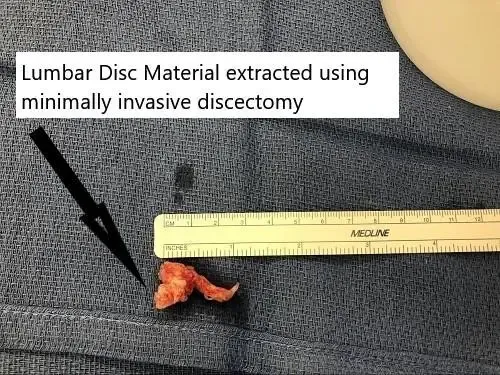
The nerve roots are carefully retracted to the other side to expose the disc herniation. The extruded disc is removed carefully. Once all the loose disc herniation is removed, the nerve roots are checked for any pressure.
After a satisfactory decompression is achieved, hemostasis is achieved and the wound is closed. We also use vancomycin antibiotics in the wound along with hemostatic agents.
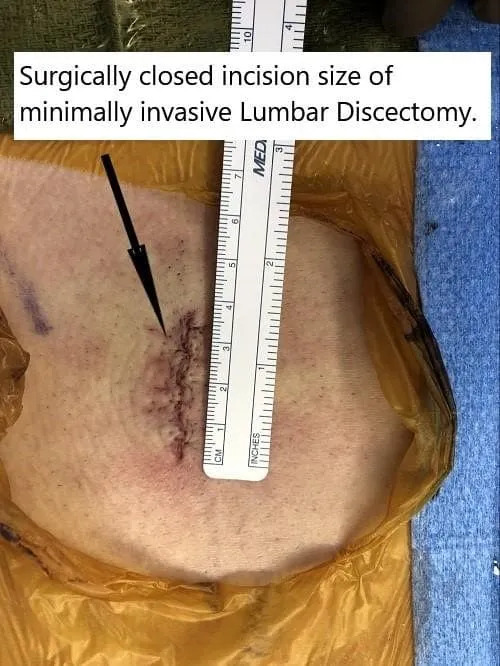
The incision for microdiscectomy is usually about 5 cm. Patients usually use a small dressing on their lower back. After the surgery, the patient is flipped onto their back and recovered from anesthesia and moved to the recovery unit.
Once they are awake and up and about, they are discharged to their home. They are sent with pain medications.

Other Problems That Can Feel Similar (Differential Diagnosis)
Conditions that may present with symptoms similar to lumbar disc herniation include:
- Piriformis Syndrome: Compression of the sciatic nerve by the piriformis muscle in the buttocks.
- Spinal Stenosis: Narrowing of the spinal canal that can mimic radiculopathy.
- Sacroiliac Joint Dysfunction: Can cause lower back pain and radiating pain down the legs.
- Muscle Strains: Often confused with nerve compression due to similar pain patterns.
Treatment Options
Non-Surgical Care
- Physical Therapy: Focuses on strengthening back muscles and improving flexibility.
- Medications: NSAIDs, muscle relaxants, or corticosteroids to reduce inflammation and pain.
- Epidural Steroid Injections: To reduce inflammation around the compressed nerves.
- Nerve Blocks: For targeted pain relief.
Surgical Care
- Microscopic Discectomy: A minimally invasive surgery using an operating microscope to remove herniated disc material.
- Endoscopic Discectomy: Uses a small camera (endoscope) and specialized instruments for even smaller incisions and faster recovery.
- Laminectomy: In cases where more extensive decompression is needed.
Recovery and What to Expect After Treatment
Postoperative care for microdiscectomy and endoscopic discectomy includes:
- Pain Management: Controlled with medications, and patients are encouraged to move soon after surgery.
- Physical Therapy: To regain strength and flexibility in the lower back.
- Hospital Stay: Most patients are discharged the same day or within 24 hours after surgery.
- Activity Restrictions: Avoiding heavy lifting or bending for several weeks to allow for healing.
Possible Risks or Side Effects (Complications)
Although the surgery is minimally invasive, there are still risks involved:
- Infection: At the surgical site.
- Nerve Injury: Rare, but can occur during the procedure.
- Dural Tear: Damage to the protective covering of the spinal cord, which may require repair.
- Hematoma: A collection of blood outside the blood vessels, which could require surgical drainage.
- Recurrent Disc Herniation: The disc could herniate again, requiring additional surgery.
Long-Term Outlook (Prognosis)
The prognosis for patients undergoing microdiscectomy or endoscopic discectomy is generally favorable, with most patients experiencing significant relief from pain and improved function. The minimally invasive nature of these procedures leads to quicker recovery times and lower complication rates compared to traditional open surgery.
Out-of-Pocket Costs
Medicare
CPT Code 63030 – Microdiscectomy: $225.06
CPT Code 62380 – Endoscopic Discectomy: $410.41
Under Medicare, 80% of the approved amount for these procedures is covered once the annual deductible has been met. The remaining 20% is typically the patient’s responsibility. Supplemental insurance plans—such as Medigap, AARP, or Blue Cross Blue Shield—generally cover this 20%, leaving most patients with little to no out-of-pocket expenses for Medicare-approved discectomy surgeries. These supplemental plans coordinate directly with Medicare to ensure full coverage for the procedures.
If you have secondary insurance—such as Employer-Based coverage, TRICARE, or Veterans Health Administration (VHA)—it serves as a secondary payer once Medicare has processed the claim. After your deductible is satisfied, the secondary plan may cover any remaining balance, including coinsurance or any uncovered charges. Most secondary insurance plans have a modest deductible, typically between $100 and $300, depending on the specific policy and network status.
Workers’ Compensation
If your lumbar spine condition requiring discectomy surgery is work-related, Workers’ Compensation will fully cover all treatment-related costs, including the procedure, hospitalization, and rehabilitation. You will have no out-of-pocket expenses under an accepted Workers’ Compensation claim.
No-Fault Insurance
If your lumbar spine injury resulting in discectomy surgery is caused by a motor vehicle accident, No-Fault Insurance will pay for all medical and surgical expenses, including microdiscectomy and endoscopic discectomy. The only possible out-of-pocket cost may be a small deductible depending on your policy terms.
Example
Lisa, a 55-year-old patient with a herniated lumbar disc, underwent microdiscectomy (CPT 63030) to relieve sciatica. Her estimated Medicare out-of-pocket cost was $225.06. For a more advanced endoscopic discectomy (CPT 62380) performed later, her estimated out-of-pocket cost was $410.41. Since Lisa had supplemental insurance through Blue Cross Blue Shield, the 20% that Medicare did not cover was fully paid, leaving her with no out-of-pocket expenses for either procedure.
Frequently Asked Questions (FAQ)
Q. How long does it take to recover from microdiscectomy or endoscopic discectomy surgery?
A. Most patients experience a significant reduction in pain and can resume normal activities within 1-2 weeks, though full recovery may take 4-6 weeks.
Q. Will I experience less pain with minimally invasive surgery compared to traditional open surgery?
A. Yes, patients generally experience less postoperative pain and discomfort, with a faster return to daily activities compared to traditional open surgery.
Q. Is the surgery successful for all patients?
A. Microdiscectomy and endoscopic discectomy are highly successful for patients with single-level disc herniations and radiculopathy. However, the outcome may vary depending on the extent of nerve damage and the presence of other conditions.
Summary and Takeaway
Microscopic and endoscopic discectomy offer a minimally invasive solution for treating lumbar disc herniation, significantly improving recovery times and reducing complications compared to traditional open surgery. These techniques have proven to be effective in relieving pain, restoring function, and allowing for a quicker return to work and normal activities.
Clinical Insight & Recent Findings
A recent study examined the initial experience of transforaminal endoscopic lumbar discectomy (TELD) in a clinical unit, highlighting its effectiveness in treating lumbar disc herniation. The study included ten male patients, with a mean age of 37.9 years.
It revealed that while preparation times remained stable, the surgical time decreased after the initial learning curve, which was identified after the fourth case. Patients showed significant improvement in their Oswestry Disability Index (ODI) scores, especially at three months post-operation, despite some initial delayed symptom relief.
The study concluded that TELD is a promising minimally invasive procedure, with a learning curve for surgeons that does not affect patient outcomes significantly. However, it emphasized that initial symptoms may resolve slowly. (“Study of transforaminal lumbar endoscopic discectomy in a single orthopedic unit – see PubMed”.)
Who Performs This Treatment? (Specialists and Team Involved)
Microscopic and endoscopic discectomy are performed by:
- Spine Surgeons: Orthopedic or neurosurgeons specializing in spinal disorders.
- Anesthesiologists: To manage anesthesia during surgery.
- Physical Therapists: To assist with rehabilitation after surgery.
When to See a Specialist?
If you experience persistent radicular pain (sciatica), numbness, or weakness in the legs that doesn’t improve with conservative treatments, you may need to consult a spine specialist to discuss the possibility of surgery.
When to Go to the Emergency Room?
Seek emergency care if you experience:
- Sudden loss of bladder or bowel control.
- Severe, unmanageable pain.
- Sudden weakness or numbness in the legs.
What Recovery Really Looks Like?
Most patients experience quick relief from pain and are encouraged to begin light activities shortly after surgery. Physical therapy is critical to strengthening the back and improving flexibility during recovery.
What Happens If You Ignore It?
Ignoring symptoms of lumbar disc herniation and nerve compression can lead to worsening pain, permanent nerve damage, and loss of mobility. Early surgical intervention often leads to better long-term outcomes.
How to Prevent It?
Maintaining a healthy weight, practicing good posture, and engaging in regular back-strengthening exercises can help prevent disc herniation and reduce the need for surgical interventions.
Nutrition and Bone or Joint Health
A diet rich in calcium and vitamin D can support bone health, while maintaining hydration and overall fitness can reduce strain on the spine.
Activity and Lifestyle Modifications
After surgery, it is important to avoid heavy lifting and high-impact activities during the recovery period. Gentle exercises, like walking and swimming, can help maintain flexibility and strength.
