
Rotator Cuff Tear
A rotator cuff tear primarily affects the middle and older age group, and can be injured in an acute event like fall or accident.
The rotator cuff tear is more commonly a chronic phenomenon in which the tear happens over the span of many years gradually progressing from a partial tear to a complete tear. These tears are usually caused due to bone spurs or osteophytes present on the undersurface of Acromion or the Acromioclavicular joint.
These bone spurs are formed because to aging as well as due to overuse of the shoulder due to daily activities or recreational activities like racquet sports, swimming, volleyball, painting etc. There may be periods of exacerbation or acute on chronic injury which may accelerate or cause completion of the tear leading to acute type of presentation.
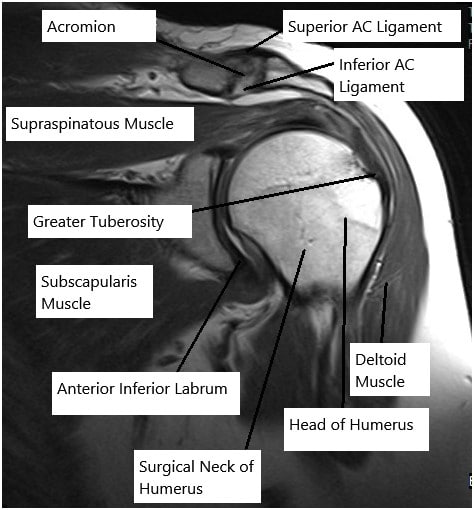
MRI of the shoulder joint
The tear may involve one or more of the tendons of the rotator cuff. Most common tendon to be involved in a rotator cuff tear is a supraspinatus tendon and infraspinatus tendon. Deficiency of rotator cuff can cause compromise in elevation as well as rotation movements and may present in the form of weakness.
DIAGNOSIS
Patients with rotator cuff tear most commonly present with chronic pain in the side and front of the shoulder which is exacerbated with movement, especially overhead elevation as well as rotation. These patients may also complain of nighttime pain, discomfort and awakenings. The patient may also complain of weakness and loss of function in the arm, in the shoulder joint. Occasionally, the patient may complain of numbness and tingling associated with pain.
In patients who present with chronic rotator cuff tear, may complain of off and on gradually worsening shoulder pain from many months to years and patients with acute presentation, patient may inform of an accidental injury with sudden onset of pain and weakness. Occasionally, the patient may present with sudden onset of complete loss of function in the arm when it is also named as pseudoparalysis. Acute rotator cuff tears are essentially found in younger population. Patients with chronic rotator cuff tear may occasional present without any pain, though will complain of weakness and loss of function.
The diagnosis of rotator cuff tear is usually suggested by certain tests that are done by the physician in the office. The tear can be confirmed with the help of advanced imaging and x-rays usually performed to rule out any bony injury as well as to look for bone spurs or osteophytes which are common under the acromion and over the acromioclavicular joint.
Confirmation of diagnosis can be done with MRI. The tear in chronic setting is usually caused due to bone spurs or osteophytes which are present on the undersurface of the acromion and over the acromioclavicular joint. These osteophytes cause reduction in space for the rotator cuff to move as well as cause impingement on digging in to the tendon leading to inflammation and partial tear and subsequently complete tear of the tendon. An MRI can help find the tear and the muscle involved as well as help in grading the tear to be partial, high grade partial or complete or only inflammation of the tendon cause tendinitis.
DIFFERENTIAL DIAGNOSIS
A rotator cuff tear may occasionally be confused with certain other conditions like acromioclavicular arthritis, impingement syndrome, cervical radiculopathy, fibromyalgia, shoulder dyskinesis, elbow pathologies like lateral or medial epicondylitis, and many more.
ROTATOR CUFF TENDINITIS
TREATMENT
Once the diagnosis is suggested or confirmed by physical examination and MRI, there are multiple options for the treatment of a rotator cuff tear.
Rotator cuff tendinitis without a tear can be usually treated with rest and anti-inflammatory medications, heat or cold compresses and with the possible use of cortisone injection in the subacromial area to decrease the inflammation. The patient can also be sent for physical therapy rehabilitation. It takes around 2 to 4 weeks to recover from rotator cuff tendinitis.
Occasionally, there can be a recurring problem and patient may need to have cortisone injections after 3 months. It is relatively safe to get 3 to 4 cortisone injections for a year at a difference of 3 or more months between the two shots. In patients with partial rotator cuff tear, patients are initially treated conservatively with anti-inflammatory medications, avoidance of activity which aggravate the pain, cortisone injection and physical therapy.
Patients with rotator cuff tear are surgical candidate though conservative treatment can be tried before going for surgery. Patients who do not improve or who have recurrence with deterioration of symptoms are suggestive of surgical option. Patients who are smokers are asked to quit smoking and avoid nicotine in any form for good healing of the cuff.
SURGICAL TREATMENT
Surgical treatment of a rotator cuff tear involves arthroscopic examination of the shoulder joint through small incisions. This surgery is usually performed on an outpatient basis. Patient is usually given a shoulder nerve block prior to the surgery. This block helps in pain relief during the surgery and for the next day after the surgery.
The patient also given general anesthesia during the surgery. Patients are placed in lateral position with supports. The shoulder joint and the rotator cuff is examined using arthroscope through small incisions. If a tear is found in the rotator cuff, it is repaired using sutures and anchors through small incisions.
The bone spurs from the acromion as well as the acromioclavicular joint if present are excised and the bone smoothened to prevent recurrence. Occasionally patient may have fraying or tearing of the biceps tendon which may need to be fixed too. Patients are given antibiotics to cover for the risk of infection in the perioperative duration.
POST OPERATIVE CARE
Patients are treated in a specialized elbow sling postoperatively. Immediately after the surgery, the patients are instructed not the use the operated extremity and keep it in sling except for shower and exercises as instructed. The patients are provided with medications in the hospital as well as for home to take care of pain. Patient may observe bruising of their arm up to the elbow or even up to the wrist after the surgery.
This is due to trickling of the blood from the surgical site along the gravity. Incisions need to be kept clean and dry. The patients are instructed to avoid bath and hot tubs, swimming, heavy lifting, driving and smoking. The patients can take shower and remove the dressings after 72 hours from surgery and replace it with dry dressing. The patients are advised to eat healthy and nutritious diet with lot of fibers.
The patients are also instructed to use over-the-counter laxatives for constipation that may develop due to pain medications. Patients are usually seen in office in 7-10 days after the surgery. They are sent for Physical Therapy at an appropriate time after the surgery for quicker recovery after the surgery to regain full range of motion and strength. Time of start of Physical Therapy is dependent on the size of the tear, surgery performed as well as many other factors.
Rotator cuff repair usually takes about 12 weeks to heal completely, but it could take more time to regain full range of motion and strength and may vary from patient to patient. Patient may have difficulty sleeping in bed immediately after the surgery and are suggested to use recliners or multiple pillows to make themselves comfortable. It may take one to three months for the patient to get comfortable in bed after the rotator cuff repair surgery.
REHABILITATION AND PHYSICAL THERAPY
Patients with rotator cuff tendinitis and partial tear as well as patient with full tear, but who do not prefer to undergo surgery are sent for physical therapy to strengthen their muscles as well as regain range of motion. Specific exercises to strengthen the rotator cuff muscles is performed under supervision as well as with home-based exercise program. The patients who undergo surgical management and repair of rotator cuff are also enrolled in physical therapy starting from 1 to 4 weeks after the surgery. Time of start of Physical Therapy is dependent on the size of the tear, surgery performed as well as many other factors.
Disclaimer – The above video content is external and shows the opinion of the involved vendor.
Larger rotator cuff tears are usually kept in sling for a month before the physical therapy is started. Patients who are smokers are asked to quit smoking and avoid nicotine in any form for good healing of the cuff. If the patient continue to smoke after the surgery, then the chances of failure are high.
Patients who have smaller tear are put into rehabilitation program early and have quicker recovery. It may take 3 to 6 months for complete recovery of rotator cuff repair. Once fully recovered, the patient will regain full range of motion and strength so as to return back to normal activities of daily living as well as recreation.
RISKS AND COMPLICATIONS
Complications are not common but can occur. It is pertinent that patients understand prior to making the decision of have this operation so you can make an informed decision on the advantages and disadvantages of surgery. These can be:
Medical (Anesthetic) complications:
Medical complications include those due to your general wellbeing and due to Anaesthesia given before and during the surgery. These include but not limited to:
Allergic reactions to medications, excessive blood loss requiring transfusion with its low risk of disease transmission, heart attack, stroke, kidney failure, pneumonia, bladder infections. Complications from nerve blocks such as infection or nerve damage. Serious medical problems can lead to ongoing health concerns, prolonged hospitalization.
Surgical Complications:
Risks of Rotator cuff repair surgery may include though not limited to:
- Infection – Patient may need to be administered prolonged antibiotics or even undergo cleaning surgery. Results are usually suboptimal in this population group.
- Deltoid detachment –This is a complication after an open repair and unusual to happen after an arthroscopic repair
- Stiffness – Despite physical therapy and patient motivation, stiffness may occur. It is treated with Physical therapy. Recalcitrant shoulder stiffness may require capsular release to regain range of motion.
- Tendon re-tear.There is a chance for re-tear following all types of repairs. The larger the tear, the higher the risk of re-tear. Smokers and patient with systemic diseases are at a higher risk for re-tear. Repeat surgery is needed only if there is severe pain or loss of function.
- Tingling and numbness
- Damage to nerves or vessels
- Hardware problems
- Residual pain
- Reflex Sympathetic Dystrophy
Some of these conditions may require hospitalization, aspiration, injections or even surgery
Factors leading to likelihood of suboptimal recovery after a rotator cuff repair:
- Poor tendon/tissue quality
- Previous failed surgeries
- Large or massive tears
- Poor patient compliance with rehabilitation and Physical Therapy
- Older than 65 years group
- Smoking and use of other nicotine products
- Workers’ compensation claims
- Postoperative infection
Certain patient population is at a higher risk for complication which include but are not limited to:
- Smoking
- Seizures
- Obstructive sleep apnea
- Obesity
- High blood pressure
- Diabetes
- Other medical conditions involving your heart, lungs or kidneys
- Medications, such as aspirin, that can increase bleeding
- History of heavy alcohol use
- Drug allergies
- History of adverse reactions to anesthesia
WHEN TO VISIT AN EMERGENCY ROOM AFTER A SURGERY:
- Suspected cardiac problem: severe chest pain or pressure, shortness of breath, tightness in chest, pain in left arm, jaw pain, dizziness or fainting, unexplained weakness or fatigue, rapid or irregular pulse, sweating, cool, clammy skin, and/or paleness
- Suspected Stroke: trouble speaking, changes in vision, confusion or other change in mental status
- Suspected venous thrombosis: swelling of the legs, ankles, or feet, discomfort, heaviness, pain, aching, throbbing, itching, or warmth in the legs, sudden shortness of breath, chest pain, coughing up blood, rapid or irregular heart rate
- Suspected Sepsis: high grade fever, with shivers associated with fatigue, dizziness, racing heart, pale or discolored skin, sleepy, difficult to rouse, confused, short of breath
- Heavy bleeding from the surgical site
- Severe allergic reaction with trouble breathing, swelling, hives
WHEN TO CONTACT A DOCTOR’S OFFICE AFTER SURGERY:
- temperature more than 101 degrees Fahrenheit
- increased pain or tenderness near the incision
- poor pain relief
- signs of infection: increased swelling, redness, increased drainage, increased warmth, pus, foul smell, bleeding at the incision, incision coming apart
- inability to feel or move fingers or toes
- pale blue, white or abnormally cold fingers or toes
- nausea (upset stomach) or vomiting (throwing up) that won’t stop
- increased tiredness
- a generally worse feeling than you had when you left the hospital
- problems urinating, severe constipation or severe diarrhea
- a concern about any other symptoms that seem unusual
SUMMARY
Rotator cuff pathologies are common and usually present with pain and weakness in overhead activities as well as in rotation. Physical examination as well as MRI can be helpful in diagnosis of pathology. Impingement syndrome, rotator cuff tendinitis and partial tears are usually treated conservatively.
Patients who fail conservative treatment as well as in patients who have complete rotator cuff tear usually need surgical treatment in the form of arthroscopic surgery and repair. The results of arthroscopic surgeries are good and reliable.

I am Vedant Vaksha, Fellowship trained Spine, Sports and Arthroscopic Surgeon at Complete Orthopedics. I take care of patients with ailments of the neck, back, shoulder, knee, elbow and ankle. I personally approve this content and have written most of it myself.
Please take a look at my profile page and don't hesitate to come in and talk.