Lumbar Degenerative Disc Disease (DDD)—also known as lumbar spondylosis—is a condition in which the intervertebral discs in the lower back undergo wear and tear over time. As part of the natural aging process, discs lose water content, flatten, and develop small tears. These changes reduce the spine’s flexibility and ability to absorb shock, sometimes leading to pain, stiffness, or nerve compression.
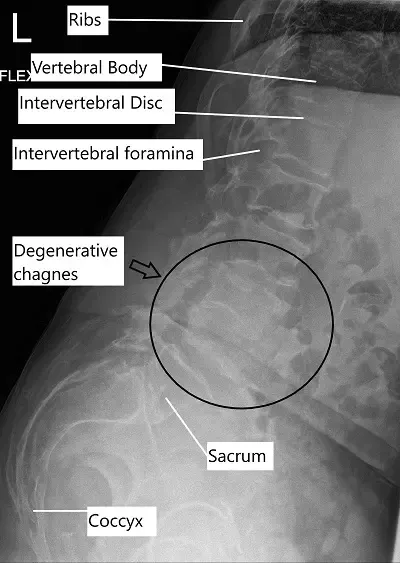
X-ray showing lumbar degenerative disc disease.
- How Common It Is and Who Gets It? (Epidemiology)Lumbar DDD is extremely common in adults over 40 and affects nearly everyone to some degree as they age. However, only a portion of individuals develop symptoms. Risk factors include genetics, repetitive strain, obesity, smoking, diabetes, and a sedentary lifestyle.Why It Happens – Causes (Etiology and Pathophysiology)The main cause of degenerative disc disease is loss of hydration in the discs, which makes them less resilient.
Contributing factors include:- Age: Natural degeneration over time.
- Repetitive motion or heavy lifting: Causes micro-injuries.
- Trauma: Injury to the lower back.
- Smoking: Reduces oxygen supply to discs.
- Systemic conditions: Diabetes or arthritis accelerate wear and tear.
- Annulus fibrosus: Tough outer ring.
- Nucleus pulposus: Soft, gel-like center.
- Lower back pain that worsens with movement or prolonged sitting.
- Pain radiating to the legs (sciatica) caused by nerve compression.
- Tingling, numbness, or weakness in the legs or feet.
- Difficulty walking or standing for long periods (neurogenic claudication).
- Relief when bending forward or sitting.
- X-rays: Show bone spurs, loss of disc height, and alignment.
- MRI: Reveals disc degeneration, nerve compression, and inflammation.
- CT scans: Provide detailed images of bone structure.
- EMG: Assesses nerve function if weakness or numbness is present.
- Mild degeneration: Early disc dehydration and minimal pain.
- Moderate degeneration: Disc height loss and facet joint arthritis.
- Severe degeneration: Bone spurs, nerve compression, or spinal stenosis.
- Herniated disc
- Lumbar spinal stenosis
- Facet joint arthritis
- Sacroiliac joint dysfunction
- Peripheral neuropathy or vascular claudication
Common treatments include:- Medications: Anti-inflammatory drugs, pain relievers, or muscle relaxants.
- Physical therapy: Strengthening core muscles, improving posture, and flexibility.
- Epidural or nerve block injections: Reduce inflammation and nerve irritation.
- Lifestyle changes: Maintaining healthy weight, avoiding smoking, and proper body mechanics.
Common surgical options include:- Discectomy: Removal of herniated or damaged disc material compressing a nerve.
- Laminectomy: Removal of part of the vertebra to relieve nerve pressure.
- Microdiscectomy or endoscopic discectomy: Minimally invasive approaches.
- Spinal fusion: Stabilizes the spine using rods, screws, and bone grafts to permanently join vertebrae.

Instruments used for bone graft insertion
The bone graft is inserted with the help of the instruments shown above during a spinal fusion surgery.
Different sizes of shavers used for removal of disc material
The shavers are used in spinal fusion surgery to remove the intervertebral disc material and create space for insertion of a bone cage along with bone graft to aid in the fusion of the involved segments.
Recovery and What to Expect After Treatment
- Non-surgical: Improvement is gradual over several weeks to months.
- After surgery: Most patients walk within a day and begin light activities within weeks.
Physical therapy plays an essential role in regaining flexibility and strength. Full recovery may take 3–6 months depending on the procedure.
Possible Risks or Side Effects (Complications)
Potential risks include:
- Infection or bleeding
- Nerve injury
- Dural tear (spinal fluid leak)
- Hardware failure or non-fusion after surgery
- Persistent pain or stiffness
Good preoperative planning and postoperative care help minimize complications.
Long-Term Outlook (Prognosis)
Most people with lumbar DDD experience excellent outcomes with conservative management or surgery when needed. Surgery often provides long-term relief from leg pain and nerve symptoms. Maintaining core strength and flexibility helps prevent recurrence.
Out-of-Pocket Costs
Medicare
CPT Code 63047 – Decompression (Lumbar Laminectomy): $271.76
CPT Code 22612 – Posterior Lumbar Fusion: $382.85
CPT Code 22558 – Anterior Lumbar Fusion (ALIF): $368.50
CPT Code 22842 – Instrumentation (Rods, Screws, Plates – 3–6 Segments): $185.26
Under Medicare, 80% of the approved cost for these spinal procedures is covered once your annual deductible has been met. Patients are responsible for the remaining 20%. Supplemental insurance plans—such as Medigap, AARP, or Blue Cross Blue Shield—typically cover this 20%, leaving patients with little to no out-of-pocket costs for Medicare-approved surgeries. These supplemental plans are designed to complement Medicare and provide full coverage for necessary spine procedures like decompression, fusion, and stabilization.
If you have secondary insurance—such as Employer-Based coverage, TRICARE, or Veterans Health Administration (VHA)—it functions as a secondary payer after Medicare. Once your deductible is satisfied, these plans may cover remaining balances, including coinsurance and uncovered costs. Deductibles for secondary insurance typically range between $100 and $300, depending on the specific policy and network of care providers.
Workers’ Compensation
If your spinal condition requiring decompression or fusion surgery resulted from a work-related injury, Workers’ Compensation will pay for all associated costs, including surgical, hospital, and rehabilitation expenses. You will have no out-of-pocket expenses under an accepted Workers’ Compensation claim.
No-Fault Insurance
If your spine injury or degenerative condition was caused or aggravated by an automobile accident, No-Fault Insurance will cover all necessary medical and surgical costs, including decompression, fusion, and instrumentation. The only potential expense may be a small deductible depending on your insurance policy terms.
Example
Thomas, a 69-year-old patient, underwent lumbar decompression (CPT 63047) and posterior spinal fusion with instrumentation (CPT 22612 + 22842) to relieve nerve compression and stabilize his spine. His total Medicare out-of-pocket costs were $271.76, $382.85, and $185.26. Because he had supplemental coverage through Medigap, the remaining 20% not covered by Medicare was fully paid, leaving him with no out-of-pocket expenses for the surgery.
Frequently Asked Questions (FAQ)
Q. What causes lumbar degenerative disc disease?
A. It’s primarily caused by age-related wear and tear of spinal discs, but smoking, repetitive strain, and injuries can accelerate the process.
Q. Can lumbar DDD cause nerve pain or sciatica?
A. Yes. As discs collapse, they may compress nearby nerves, causing radiating leg pain, numbness, or tingling.
Q. When should surgery be considered?
A. Surgery is recommended when pain persists for more than 3 months despite conservative therapy or if neurological deficits worsen.
Q. Can lifestyle changes help manage lumbar DDD?
A. Absolutely. Regular exercise, good posture, quitting smoking, and maintaining a healthy weight significantly reduce symptoms and slow progression.
Summary and Takeaway
Lumbar Degenerative Disc Disease is a natural part of aging that causes lower back and leg pain due to disc dehydration and joint wear. Most patients improve with conservative care. For persistent cases, modern surgical options—such as decompression or spinal fusion—provide effective pain relief and restore function. Maintaining a strong, flexible spine through exercise and healthy habits prevents recurrence.
Clinical Insight & Recent Findings
A recent systematic review analyzed 20 clinical and experimental studies to evaluate the effects of exercise-based rehabilitation for patients with lumbar degenerative disc disease. The findings demonstrated that structured physical therapy interventions such as hydrotherapy, core stability exercises, Pilates, and suspension training significantly reduced pain, improved range of motion, and enhanced quality of life.
Among the various approaches, suspension training and aquatic therapy showed the most consistent benefits, producing superior outcomes in both pain reduction and functional performance compared with standard core stabilization programs. Pilates and yoga were also effective, showing comparable results to conventional rehabilitation, while combined exercise and massage protocols further improved physical function.
Despite these positive outcomes, the review noted limitations such as small sample sizes, heterogeneous study designs, and short follow-up durations. Overall, exercise-based rehabilitation was identified as a safe and effective strategy for managing lumbar degenerative disc disease, with multimodal programs offering the greatest benefit. (Study of exercise-based rehabilitation for lumbar degenerative disc disease – See PubMed.)
Who Performs This Treatment? (Specialists and Team Involved)
Care is provided by orthopedic spine surgeons or neurosurgeons, along with physical therapists, pain management specialists, and rehabilitation experts.
When to See a Specialist?
You should see a spine specialist if you have:
- Persistent back or leg pain lasting over six weeks
- Numbness, tingling, or weakness in the legs
- Difficulty walking or standing for long periods
- Pain relief when leaning forward
When to Go to the Emergency Room?
Seek emergency care if you experience:
- Sudden loss of bladder or bowel control
- Severe or worsening leg weakness
- Fever, unexplained weight loss, or trauma-related pain
What Recovery Really Looks Like?
Recovery may vary depending on treatment. Most patients return to normal activity gradually, with full recovery after 3–6 months. Consistent physical therapy and healthy posture habits are key for long-term success.
What Happens If You Ignore It?
Ignoring lumbar DDD can lead to chronic pain, worsening nerve compression, or spinal deformity. Severe cases may cause permanent nerve damage or paralysis if untreated.
How to Prevent It?
- Maintain good posture and ergonomics.
- Exercise regularly to strengthen core muscles.
- Avoid smoking and excessive weight gain.
- Practice safe lifting techniques.
Nutrition and Bone or Joint Health
A balanced diet rich in calcium, vitamin D, and omega-3 fatty acids supports spinal health. Staying hydrated keeps spinal discs flexible and healthy.
Activity and Lifestyle Modifications
Low-impact activities such as swimming, yoga, and walking help strengthen back muscles and reduce stiffness. Avoid prolonged sitting, twisting, and heavy lifting. Regular stretching keeps the spine flexible and pain-free.
Do you have more questions?
What causes Lumbar Degenerative Disc Disease?
LDDD is caused by the natural aging process, where the intervertebral discs lose hydration and become less elastic, leading to degeneration.
What are the symptoms of Lumbar Degenerative Disc Disease?
Symptoms include back pain, leg pain, tingling, numbness, and sometimes weakness in the legs or feet.
How is LDDD diagnosed?
Diagnosis typically involves physical examination, patient history, and imaging studies like X-rays, MRI, and sometimes CT scans.
What conservative treatments are available for LDDD?
Conservative treatments include physical therapy, pain medications, lifestyle modifications, and possibly nerve blocks.
Can LDDD be prevented?
While aging is inevitable, maintaining a healthy lifestyle, avoiding smoking, and practicing good posture can help slow the progression.
When should surgery be considered for LDDD?
Surgery is considered when conservative treatments fail, or if there are significant neurological deficits or severe pain affecting quality of life.
What types of surgeries are available for LDDD?
Surgeries include discectomy, decompression laminectomy, and various types of spinal fusion surgeries.
What is a discectomy?
A discectomy involves removing part of a damaged disc to relieve pressure on a nerve.
What is spinal fusion?
Spinal fusion involves joining two or more vertebrae to stabilize the spine and reduce pain.
Are there minimally invasive options for LDDD surgery?
Yes, minimally invasive options like microdiscectomy and endoscopic discectomy are available.
What are the risks of LDDD surgery?
Risks include infection, nerve damage, bleeding, failure of the fusion, and complications from anesthesia.
What is the recovery time after LDDD surgery?
Recovery time varies but generally ranges from a few weeks to several months, depending on the type of surgery and the patient’s overall health.
How effective is surgery for LDDD?
Surgery can be highly effective, especially for patients with radicular symptoms or neurological claudication.
Can LDDD recur after surgery?
While surgery can relieve symptoms, it does not cure the underlying degenerative process, so recurrence is possible.
What lifestyle changes can help manage LDDD?
Regular exercise, maintaining a healthy weight, avoiding smoking, and practicing good posture can help manage symptoms.
Is physical therapy helpful for LDDD?
Yes, physical therapy can strengthen the muscles around the spine, improve flexibility, and reduce pain.
Can medications help with LDDD pain?
Yes, medications like NSAIDs, muscle relaxants, and sometimes opioids can help manage pain.
What is radiculopathy?
Radiculopathy is pain, numbness, or weakness radiating along a nerve due to compression or irritation at its root.
What is lumbar canal stenosis?
Lumbar canal stenosis is the narrowing of the spinal canal in the lower back, often causing pain and neurological symptoms.
What is the prognosis for patients with LDDD?
The prognosis varies; many patients experience stable symptoms with periods of exacerbation, and a small subset may develop significant issues.
Can LDDD lead to permanent nerve damage?
In severe cases, untreated LDDD can lead to permanent nerve damage.
Is there a genetic component to LDDD?
Genetics can play a role, with some individuals being more predisposed to disc degeneration.
How does smoking affect LDDD?
Smoking accelerates disc degeneration by reducing blood flow to the discs and impairing healing.
What is cauda equina syndrome and how is it related to LDDD?
Cauda equina syndrome is a rare but serious condition where nerve roots at the lower end of the spinal cord are compressed, often requiring urgent surgical intervention.
