Sciatica, or lumbar radiculopathy, is a condition characterized by pain radiating from the lower back into the legs, often accompanied by tingling, numbness, or weakness. The pain typically follows the distribution of the affected nerve root, commonly along the outer thigh, leg, and foot. This pain may occur unilaterally or bilaterally, depending on which nerve root is involved.

MRI of the lumbar spine in sagittal section showing herniated L5-S1 intervertebral disc.
How Common It Is and Who Gets It? (Epidemiology)
Sciatica is a common condition, with a lifetime prevalence of approximately 40%. It most often affects individuals between the ages of 30 and 50. Risk factors include aging, degenerative spinal conditions, obesity, and a sedentary lifestyle. Sciatica is more prevalent in men than women and is frequently associated with occupations that involve heavy lifting or prolonged sitting.
Why It Happens – Causes (Etiology and Pathophysiology)
The most common cause of sciatica is a herniated lumbar disc, where the disc material presses on the nerve root. Other causes include degenerative changes such as facet arthritis, spinal stenosis, or osteophyte formation. Sciatica can also result from synovial cysts or trauma. These conditions irritate or compress the nerve roots, leading to inflammation, ischemia, and pain.
How the Body Part Normally Works? (Relevant Anatomy)
The spine consists of vertebrae separated by intervertebral discs, which cushion and stabilize the spine. The nerve roots exit the spinal cord through the intervertebral foramen. The lumbar spine, in particular, is prone to disc herniation due to its weight-bearing function. The sciatic nerve, originating from the lumbar and sacral spinal roots, runs through the pelvis and down the legs, providing motor and sensory function.
What You Might Feel – Symptoms (Clinical Presentation)
Patients with sciatica often experience pain radiating from the lower back to the leg, typically following a specific dermatome. This pain can range from mild to severe and may be accompanied by tingling, numbness, and, in some cases, weakness in the affected leg. Symptoms are exacerbated by prolonged sitting, bending, or lifting.
How Doctors Find the Problem? (Diagnosis and Imaging)
Diagnosis is typically clinical, based on a patient’s history and physical examination. Imaging tests like MRI are crucial for identifying disc herniations, degenerative changes, and other structural abnormalities in the lumbar spine. MRI scans in sagittal and axial views provide detailed images of the disc space, nerve roots, and the surrounding structures, helping guide treatment decisions.
Classification
Sciatica can be classified based on the underlying cause of the symptoms. Herniated disc-related sciatica is the most common type, but other causes include degenerative disc disease, spinal stenosis, and spondylolisthesis. The severity of the symptoms can range from mild discomfort to severe, debilitating pain with associated neurological deficits.
Other Problems That Can Feel Similar (Differential Diagnosis)
Conditions that can mimic sciatica include piriformis syndrome, lumbar muscle strain, and peripheral neuropathy. Additionally, other causes of lower back pain, such as sacroiliac joint dysfunction, can present with symptoms similar to sciatica.
Treatment Options
Non-Surgical Care
Non-surgical management includes medications such as nonsteroidal anti-inflammatory drugs (NSAIDs), muscle relaxants, and anticonvulsants like gabapentin. Physical therapy, acupuncture, and chiropractic care can also help alleviate symptoms. Steroid injections, such as epidural steroid injections or selective nerve root blocks, are sometimes used for more severe cases.
Surgical Care
Surgery is considered when conservative treatments fail or if there is significant neurological impairment. Surgical options include discectomy (removal of the herniated disc), microdiscectomy (minimally invasive surgery), and endoscopic discectomy. For patients with additional spinal instability, fusion surgery may be required.
MICRODISCECTOMY/ENDOSCOPIC DISCECTOMY
Discectomy can be either open or with the use of a microscope, also known as microdiscectomy. When discectomy is done with the use of endoscopy, then it is called endoscopic discectomy.
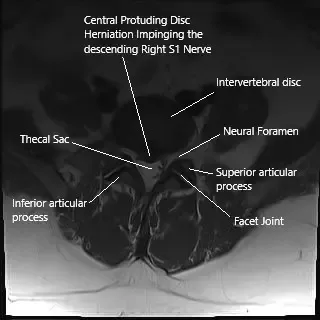
Axial section of the spine on MRI showing herniated intervertebral disc.
With the development of state of art instrumentation and better optics allowing visualization of magnification with the use of lens, microscope and endoscope, we are able to perform the surgery through smaller incisions allowing full recovery with minimal loss of blood, small incision and minimal morbidity.
In patients with isolated lumbar disc herniation without instability, microdiscectomy is the gold standard procedure in patients. This will also include decompressing the foramen and removing a part of lamina (foraminotomy and laminotomy).
Patients who have compression in the centers and bilateral disc herniations may need either procedure on both sides or removal of complete lamina (laminectomy) to allow for decompression.
For microdiscectomy, procedure is performed usually through a small incision less than 5 cm. A microscope is used for magnification and improved visualization with good illumination. The bone from the back of the spine, that is the lamina is removed to achieve a window to work (laminotomy) through which the disc can be reached and removed. The foramina was also cleared (foraminotomy).
In patients who have instability of the spinal segment, fusion surgery is performed. The bones are roughened (decorticated) and screws and rods are inserted so as to allow stability and healing and fusion to happen. Sometimes biologics like autogenous bone graft, allogeneic bone graft, substitutes like calcium triphosphate or stimulants like bone morphogenic protein or BMP can be used to enhance the fusion.
Patients who undergo microdiscectomy, foraminotomy, laminotomy, laminectomy can usually go home the same day or within 24 hours. These patients usually heal and recover faster and can be back to usual activity within 3 to 6 weeks. Patients who undergo fusion surgery take a longer recovery period and are usually in the hospital for 2 to 4 days.
Recovery and What to Expect After Treatment
Patients who undergo non-surgical treatments typically experience improvement within 6 to 12 weeks. Those undergoing microdiscectomy or other decompression procedures can generally return to normal activities within 3 to 6 weeks. Patients undergoing fusion surgeries face a longer recovery period, typically 4 to 12 weeks, depending on the procedure’s complexity.
Possible Risks or Side Effects (Complications)
As with any surgery, spinal procedures carry risks, including infection, bleeding, nerve injury, and the potential for recurrent herniation. Fusion surgeries may result in nonunion or instability. Other risks include injury to the spinal cord, blood clots, and complications related to anesthesia or general health.
Long-Term Outlook (Prognosis)
The prognosis for sciatica depends on the underlying cause and the success of the treatment. Most patients with herniated discs improve with conservative treatment or surgical intervention, with many returning to normal activities. However, some individuals may experience recurring episodes of pain or long-term discomfort, particularly those who have not undergone surgical intervention.
Out-of-Pocket Costs
Medicare
CPT Code 63030 – Microdiscectomy: $225.06
CPT Code 62380 – Endoscopic Discectomy: $410.41
Under Medicare, 80% of the approved amount for these procedures is covered once the annual deductible has been met. The remaining 20% is typically the patient’s responsibility. Supplemental insurance plans—such as Medigap, AARP, or Blue Cross Blue Shield—generally cover this 20%, leaving most patients with little to no out-of-pocket expenses for Medicare-approved discectomy surgeries. These supplemental plans work directly with Medicare to ensure full coverage for the procedures.
If you have secondary insurance—such as Employer-Based coverage, TRICARE, or Veterans Health Administration (VHA)—it serves as a secondary payer once Medicare processes the claim. After your deductible is satisfied, these secondary plans may cover any remaining balance, including coinsurance or any uncovered charges. Secondary plans typically have a modest deductible, usually between $100 and $300, depending on the specific policy and network status.
Workers’ Compensation
If your lumbar spine condition requiring discectomy surgery is work-related, Workers’ Compensation will fully cover all treatment-related costs, including surgery, hospitalization, and rehabilitation. You will have no out-of-pocket expenses under an accepted Workers’ Compensation claim.
No-Fault Insurance
If your lumbar spine injury resulting in discectomy surgery is caused by a motor vehicle accident, No-Fault Insurance will cover all medical and surgical expenses, including microdiscectomy and endoscopic discectomy. The only possible out-of-pocket cost may be a small deductible depending on your policy terms.
Example
Sarah, a 60-year-old patient with a herniated lumbar disc, underwent microdiscectomy (CPT 63030) and later endoscopic discectomy (CPT 62380). Her estimated Medicare out-of-pocket cost was $225.06 for the microdiscectomy and $410.41 for the endoscopic procedure. Since Sarah had supplemental insurance through Blue Cross Blue Shield, the 20% that Medicare did not cover was fully paid, leaving her with no out-of-pocket expenses for the surgeries.
Frequently Asked Questions (FAQ)
Q. What is the recovery time for microdiscectomy?
A. Most patients recover within 3 to 6 weeks after a microdiscectomy, though it can take longer for those who undergo fusion surgery.
Q. Can sciatica be treated without surgery?
A. Yes, many patients improve with non-surgical treatments such as physical therapy, medications, and steroid injections.
Q. What is the cost of sciatica surgery?
A. The cost of sciatica surgery can vary. For example, the estimated out-of-pocket cost for a microdiscectomy is around $225.06.
Summary and Takeaway
Sciatica is a common condition that can significantly impact quality of life. While many cases improve with conservative treatment, surgical options like microdiscectomy or endoscopic discectomy may be necessary for severe or persistent symptoms. Patients typically recover well from surgery, though the recovery time may vary depending on the procedure.
Clinical Insight & Recent Findings
A recent study developed a “people-like-me” approach to predict individual recovery outcomes for patients undergoing lumbar microdiscectomy combined with postoperative physical therapy for lumbar radiculopathy.
This approach, utilizing historical data from similar patients, demonstrated enhanced precision by integrating preoperative data with three months of postoperative data. The model significantly improved predictions for leg pain and disability at 12 months, with a 23%–43% increase in prediction accuracy compared to preoperative-only models.
This method highlights the potential for personalized prognosis, allowing clinicians to adjust treatment plans and expectations. It provides a more reliable forecast for recovery, improving patient engagement and motivation for rehabilitation (“Study on lumbar microdiscectomy recovery prediction – see PubMed”).
Who Performs This Treatment? (Specialists and Team Involved)
Sciatica treatment, including both surgical and non-surgical options, is typically managed by spine specialists such as orthopedic surgeons, neurosurgeons, and pain management specialists. A multidisciplinary team may also be involved, including physical therapists, anesthesiologists, and rehabilitation specialists.
When to See a Specialist?
You should see a specialist if your sciatica symptoms persist for more than 6 weeks, if the pain is severe, or if you experience neurological deficits such as weakness, numbness, or bowel or bladder dysfunction.
When to Go to the Emergency Room?
Seek emergency care if you experience sudden weakness in the legs, loss of bowel or bladder control, or severe, unrelenting pain that does not respond to medication.
What Recovery Really Looks Like?
Most patients recover fully within 3 to 6 weeks after a microdiscectomy. However, if you have fusion surgery, the recovery process will be longer and may involve more intensive rehabilitation.
What Happens If You Ignore It?
If left untreated, sciatica can lead to chronic pain, permanent nerve damage, and long-term disability. Early intervention typically leads to better outcomes.
How to Prevent It?
Maintaining good posture, avoiding prolonged sitting, and engaging in regular exercise can help prevent sciatica. Strengthening the core and maintaining a healthy weight are also important for spinal health.
Nutrition and Bone or Joint Health
Eating a diet rich in calcium, vitamin D, and other nutrients that support bone health can help prevent degenerative spinal conditions. Proper hydration and a balanced diet are key to maintaining overall spinal function.
Activity and Lifestyle Modifications
To manage sciatica, avoid heavy lifting and activities that put stress on the spine. Regular low-impact exercises such as walking or swimming can help strengthen the back muscles and reduce the risk of recurrence.
Do you have more questions?
How do I know if my sciatica is severe enough to require surgery?
Surgery is generally considered if you have severe, persistent pain that has not responded to at least 6 weeks of conservative treatments, such as physical therapy, medications, or injections, and if the pain significantly interferes with your daily activities.
How effective is surgery in treating sciatica?
Surgery is highly effective in providing relief from leg pain associated with sciatica, especially in the short to medium term. Many patients experience significant improvement in pain and function within weeks of the procedure.
Will my sciatica symptoms return after surgery?
While surgery often provides long-lasting relief, some patients may experience a recurrence of symptoms, especially if there are ongoing degenerative changes in the spine.
What is the recovery time after sciatica surgery?
Recovery time varies depending on the type of surgery, but most patients can return to light activities within a few weeks. Full recovery, including a return to more strenuous activities, can take several months.
Can sciatica be treated without surgery?
Yes, many cases of sciatica can be successfully managed with non-surgical treatments, including physical therapy, medications, epidural steroid injections, and lifestyle modifications.
What are the chances that non-surgical treatments will fail?
Non-surgical treatments are effective for many people, but if there is significant nerve compression, these treatments might not provide sufficient relief, leading to the consideration of surgery.
How does sciatica surgery differ from other back surgeries?
Sciatica surgery, such as a discectomy or microdiscectomy, specifically targets the removal of the disc material or bone pressing on the sciatic nerve, unlike other back surgeries that may address broader spinal issues.
Will I need to stay in the hospital after sciatica surgery?
Most sciatica surgeries, especially minimally invasive ones, are done on an outpatient basis, allowing you to go home the same day. However, in some cases, an overnight stay may be required.
Is sciatica surgery covered by insurance?
Most insurance plans cover sciatica surgery, especially if conservative treatments have been tried and failed. It’s important to check with your insurance provider for specific coverage details.
Can sciatica cause permanent nerve damage if left untreated?
Yes, in severe cases, prolonged nerve compression can lead to permanent nerve damage, resulting in chronic pain, numbness, or weakness in the affected leg.
What are the alternatives to surgery for managing sciatica?
Alternatives include physical therapy, chiropractic care, acupuncture, epidural steroid injections, and lifestyle modifications. These approaches can be effective, especially when combined.
How is the success of sciatica surgery measured?
Success is typically measured by the reduction or elimination of leg pain, improvement in function and quality of life, and the ability to return to normal activities without significant limitations.
What are the signs that I might need a reoperation after sciatica surgery?
Signs that might indicate the need for reoperation include the return of severe pain, new or worsening symptoms, or the development of complications like infection or spinal fluid leaks
Can I travel shortly after sciatica surgery?
It’s advisable to wait at least a few weeks before traveling, especially if it involves long periods of sitting. Discuss your travel plans with your surgeon to ensure it’s safe based on your recovery progress.
The content on this page has been authored, edited, or approved by the doctors below, and was last reviewed for accuracy on December 5, 2025.
