Carpal tunnel syndrome is a condition that may occur when the median nerve, a major provider of sensation to volar radial side of your hand and fingers, becomes compressed within the carpal tunnel.
The floor of carpal tunnel is formed by the eight wrist (carpal) bone and the top is transverse carpal ligament. The tunnel acts as a passageway at your wrist through which the median nerve and nine tendons (thumb and four fingers) pass to reach your hand.
Compression of the median nerve, which occurs due to a decrease in the space inside the tunnel, may be caused by conditions such as swelling of the tissue lining the tunnel (flexor tenosynovitis), fluid retention (pregnancy, thyroid disease etc.), presence of ganglion cyst, an abnormal muscle structure (proximal lumbrical origin, anomalous flexor pollicis longus slip etc.) or other conditions. In many instances, the cause is unknown (40%).
Symptoms of Carpal Tunnel Syndrome
You may feel as though your hand is “going to sleep.” Usually, your index and middle fingers are most affected, but the sensation may occur throughout your hand.
If the symptoms began recently, you may be awakened from sleep with numbness, tingling or pain, which may be relieved when you shake or rub your hand. In later stages, the numbness may become continuous.
You may also feel weakness of thumb and worse when you try to do repetitive work or try to open the jar or can.
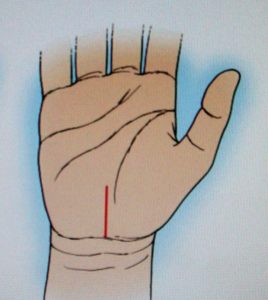
Structure of the Carpal Tunnel
Diagnosing Carpal Tunnel Syndrome
Patient history—pain, paresthesia, numbness and tingling over distribution of median nerve, thumb, index finger, middle and ring finger.
Symptoms are often worse at night (nocturnal awakening) and are aggravated by activities that requires a fixed position of the wrist such as holding a telephone or hairbrush, typing, driving a car.
Without appropriate treatment, patients with more advanced CTS complained of difficulty of opening jars or manipulating shirt buttons. Patients with basal joint arthritis also complained of difficulty of opening jars which required differential diagnosis.
Physical examination—Although sensory complaints are the hallmark of CTS, patients with milder neuropathy frequently do not have any objective abnormalities on examination.
The sensory examination may include both threshold tests (Semmes-Weinstein monofilament and vibrometry) and innervations density tests (static and moving two-point discrimination), with the former more sensitive than the latter.
Other specific provocative tests that frequently used by clinician in diagnosing CTS including the Tinel test, Phalen test, and Durkan test. Motor deficit occurred after significant sensory impairment.
The most commonly affected and sensitive motor finding is weakness of APB muscle, innervated purely by median nerve, occurred in more chronic disease. Thenar muscle atrophy is a relatively rare and may be present with more severe or end-stage of neuropathy.
Your physician will perform a physical examination to evaluate the possibility of carpal tunnel syndrome and to rule out other probable causes of median nerve compression due to thoracic outlet syndrome (TOC) or pronator teres syndrome (Double Crush Syndrome).
Electrodiagnostic testing—This is commonly performed in the evaluation of CTS include both the nerve conduction velocity (NCV) and electromyography (EMG). The distal motor latency more than 4.5 msec or more than 1 msec compared to opposite side are abnormal.
The distal sensory latency (index finger to wrist) more than 3.5 msec or o.5 msec more compared to the opposite side. The sensitivities of NCV on diagnosis of CTS are around 49% and 84% with specificities of 95% and 99%.
EMG of thenar muscle may reveal recruitment pattern, fibrillation, and positive sharp waves in severe median nerve dysfunction. Nerve conduction studies and electromyography (NCV/EMG) may be used to confirm the diagnosis and evaluate the severity of your condition.
Imaging—Plain radiograph may sometimes obtain during the work-up of patients with CTS. Ultrasound and MRI can be used to accurately determine the dimensions of the carpal tunnel and the space available for the median nerve.
However, the diagnosis of CTS remains predominantly a clinical diagnosis and adjunctive imaging studies are rarely necessary.
Treating Carpal Tunnel Syndrome
In most cases, your treatment will begin with nonsurgical approaches that may relieve your symptoms. Many patients get relief from simply modifying their activities to reduce pressure within the carpal tunnel and wearing a wristlet only at night to keep their wrist in a neutral position, not in functional position, because functional position of wrist is 30 degrees dorsiflexion.
A steroid injection may also be used to relieve symptoms (overall recurrence rate: 8-94%). Taking medications by mouth, such as vitamin B6 or nonsteroidal anti-inflammatory drug (NSAID) may be tried for some patients to relieve symptoms due to synovitis or arthritis.
If the nonsurgical methods are unsuccessful, surgery may be recommended. The goals of surgery are to reduce pressure within the carpal tunnel to alleviate median nerve compression by release transverse carpal ligament (TCL), or flexor synovectomy, or combined both methods.
The surgeries can be open, mini-open (incision about 2 cm) or endoscopic method. Endoscopic release of carpal tunnel carries the risk of cutting of the median nerve, which is a devastating complication.
Anesthesia types include General Anesthesia, Regional Nerve Block with or without IV Sedation, IV Regional Block (Bier Block) and WALANT (Wide Awake Local Anesthesia No Tourniquet).
I prefer mini-incision carpal tunnel release to avoid long incision and complications caused by endoscope surgery.
I use Regional Block and IV Sedation with tourniquet. So, I can see truly clear all the important structures of carpal tunnel region and perform successful and thorough carpal tunnel release and flexor tendon synovectomy, if necessary, for my patients. Outcomes are particularly good.
Postoperative Care —-After carpal tunnel release, we will put on short arm splint for 2 weeks to allow complete rest of wrist joint and avoid incidental injury of wrist region and nerve. Because, after release, the median nerve function comes back.
The wrist region will be hypersensitive to touch or injury. Complete protection with wrist splint is the best policy. You must do range of motion (ROM) of the fingers of surgical hand to prevent finger stiffness.
Come back to our office after 2 weeks for removal of stitches and put on steri-strip. The skin edge may be uneven due to thick palmar skin of hand. Continue wrist brace for 4 weeks during work or at night (up to your convenience or feel).
Median nerve recovery takes about 8 weeks to 6 months to recover. During this period, you may experience some burning sensation over incision wound region, numbness and tingling and weakness of hand. But the symptoms will improve gradually.
You will be off work or one hand duty for 2 weeks. (Some patients recovered more quickly, then can go back to work earlier or even next day with splint protection, just like one of my PA which I operated.)
Then light duty of surgical hand less than 5 lbs for one month. Full activity with no restriction 6 to 8 weeks after surgery.
Do you have more questions?
What is carpal tunnel syndrome?
Carpal tunnel syndrome is a condition where the median nerve is compressed as it passes through the carpal tunnel in the wrist, leading to symptoms like numbness, tingling, and pain in the hand.
What causes carpal tunnel syndrome?
It’s typically caused by repetitive hand movements, wrist anatomy, certain health conditions (like diabetes, rheumatoid arthritis), and sometimes
What are the symptoms of carpal tunnel syndrome?
Symptoms include numbness, tingling, and pain in the fingers or hand, often noticeable at night or while holding objects.
How is carpal tunnel syndrome diagnosed?
Diagnosis involves a physical examination, discussing symptoms, and may include nerve conduction studies to measure the electrical conduction of the median nerve.
What are the initial treatments for carpal tunnel syndrome?
Non-surgical treatments include wrist splinting, anti-inflammatory medications, and corticosteroid injections.
When is surgery recommended for carpal tunnel syndrome?
Surgery is recommended when symptoms are severe, persistent, and do not respond to conservative treatments.
What is open carpal tunnel release surgery?
This traditional surgery involves a larger incision in the palm to cut the ligament pressing on the median nerve to relieve pressure.
What is endoscopic carpal tunnel release surgery?
A less invasive procedure that uses a tiny camera to guide a small instrument through a smaller incision to cut the ligament.
How do I know which surgery is right for me?
The choice depends on the severity of your symptoms, your general health, lifestyle needs, and personal preference, often discussed with your surgeon.
What are the risks of open carpal tunnel release surgery?
Risks include infection, nerve damage, scarring, and sometimes incomplete symptom relief.
What are the risks of endoscopic carpal tunnel release surgery?
Similar to open surgery with additional risks like incomplete release of the ligament and transient nerve irritation from the instruments used.
What is the recovery time for open carpal tunnel surgery?
Recovery can take several weeks, with gradual improvement in symptoms and hand function.
What is the recovery time for endoscopic carpal tunnel surgery?
Recovery is generally quicker than open surgery, often with less pain and a faster return to normal activities.
What kind of pain relief can I expect after surgery?
Most patients experience significant relief from night pain and tingling immediately after surgery, with gradual improvement in other symptoms.
How long do the effects of surgery last?
The effects of surgery are generally long-lasting, with most patients experiencing permanent relief from the original symptoms.
Will I need physical therapy after surgery?
Some patients may benefit from physical therapy to regain strength and flexibility in the hand and wrist.
What are the success rates of carpal tunnel surgery?
The success rate is very high, with over 90% of patients experiencing significant relief from symptoms.
Can carpal tunnel syndrome come back after surgery?
It’s rare, but symptoms can recur, especially if underlying causes such as repetitive hand use are not addressed.
How can I prevent carpal tunnel syndrome?
Prevention strategies include ergonomic adjustments, regular breaks during repetitive tasks, hand and wrist exercises, and maintaining overall good health.
Are there lifestyle changes I can make to improve symptoms?
Yes, maintaining a healthy weight, managing chronic diseases, avoiding repetitive strain, and using ergonomic tools can help.
What are the latest advancements in carpal tunnel surgery?
Advancements include more refined endoscopic techniques and instruments that allow for smaller incisions and potentially faster recoveries.
How does carpal tunnel surgery improve hand function?
By relieving the pressure on the median nerve, surgery allows for the return of normal sensation and strength in the hand, improving overall function.
Are there any non-surgical alternatives that are effective?
Besides splinting and injections, lifestyle changes, ergonomic interventions, and some alternative therapies like acupuncture have been found helpful.
What should I expect during the surgery?
Expect a brief procedure (usually under an hour) that can be done under local anesthesia; you may go home the same day.
How soon can I return to work after carpal tunnel surgery?
Return to work depends on the type of surgery and your job type; it can range from a few days to several weeks, especially if your job involves heavy hand use.
What is carpal tunnel syndrome?
Carpal tunnel syndrome is a condition where the median nerve is compressed as it passes through the carpal tunnel in the wrist, leading to symptoms like numbness, tingling, and pain in the hand.