A selective nerve root block (SNRB) is a diagnostic and therapeutic procedure used to treat radiculopathy, often referred to as sciatica. Radiculopathy typically occurs when a nerve root is compressed, leading to pain radiating from the back or buttocks down the thigh, calf, and sometimes the foot. It may also be accompanied by tingling, numbness, or weakness in the affected leg.
Functional Anatomy
The sciatic nerve originates from the lower spine, where the lumbar and sacral nerve roots (L4, L5, S1, S2, and S3) exit the vertebral column. Compression of these nerve roots, often caused by conditions like herniated discs or degenerative stenosis, leads to symptoms of radiculopathy, including pain along the leg.
Selective nerve root block targets the specific nerve root believed to be causing the symptoms. By injecting a mixture of local anesthetic and steroid medication near the affected nerve root, the procedure aims to relieve pain and reduce inflammation.
Biomechanics or Physiology
The procedure works by targeting the nerve root, where compression or irritation is occurring. The steroid medication used during the block reduces inflammation around the nerve root, providing pain relief. The local anesthetic provides immediate but temporary relief, while the steroid works more slowly to decrease swelling and inflammation, potentially offering longer-lasting pain relief.
The effectiveness of an SNRB lies in its ability to precisely target the source of pain, offering symptomatic relief while also providing diagnostic information about the level of nerve involvement.
Common Variants and Anomalies
Patients who suffer from radiculopathy typically experience pain on one side of the body, although in cases like lumbar canal stenosis, bilateral symptoms may occur. In these cases, selective nerve root blocks can be applied to multiple levels or sides, depending on the number of nerve roots involved.
SNRBs are particularly effective when it is unclear which nerve root is causing the symptoms. It allows physicians to isolate the specific level of compression and helps guide treatment decisions such as further conservative care or surgical interventions.
Clinical Relevance
For patients who have failed conservative treatment, including medications, rest, and physical therapy, selective nerve root blocks are a valuable option. They can provide pain relief, assist in diagnosing the exact level of nerve compression, and offer temporary relief that allows the body to heal naturally.
If the pain persists, surgical options such as discectomy or decompression may be considered. Additionally, SNRBs are effective in patients with multilevel stenosis or degenerative spine disease, where diagnosing the exact level of compression is crucial for surgical planning.
Imaging Overview
X-rays and MRI scans are often used to identify the level of nerve root compression. These imaging techniques help confirm the location and severity of herniated discs, spinal stenosis, or facet joint hypertrophy that may be causing radiculopathy. Once the level of compression is identified, selective nerve root blocks can be performed with the help of fluoroscopy or CT guidance to accurately direct the needle to the affected nerve root.
Associated Conditions
Radiculopathy is commonly caused by a variety of spinal conditions, including:
- Herniated discs – where disc material compresses nerve roots.
- Spinal stenosis – narrowing of the spinal canal or foramina leading to nerve compression.
- Degenerative disc disease – the wear and tear of spinal discs.
- Facet joint hypertrophy – enlargement of facet joints that can encroach on nerve roots.
These conditions can all benefit from selective nerve root blocks as part of a comprehensive treatment plan.
Surgical or Diagnostic Applications
SNRBs are used both diagnostically and therapeutically. Diagnostic applications include confirming which nerve root is causing symptoms, especially in cases of multilevel stenosis or degenerative changes in the spine. Therapeutically, SNRBs help reduce pain, provide immediate relief through local anesthesia, and decrease inflammation with steroids, allowing for better mobility and an improved quality of life.
When used diagnostically, the procedure can help identify the precise level of nerve involvement, which is essential when considering further treatments or surgical options.
The Procedure
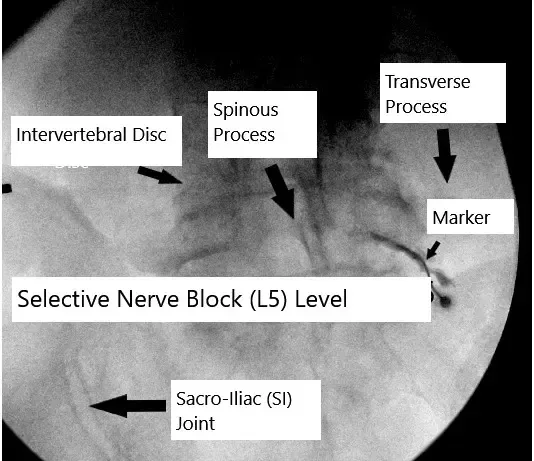
Selective nerve root blocks are performed in an operative suite. It is performed in a prone (lying on the belly) position and the patient is usually sedated. Local anesthesia is given and image intensifier or intraoperative X rays are used to direct the needle to the exact spot.
The location is checked by injecting a little amount of dye before injecting the mixture of steroid and local anesthetic. Care is taken not to inject into any adjacent vital structures. Patients are usually discharged from the operating area within a couple of hours after the procedure.
They are allowed to walk and continue with activities of daily living. There may be some worsening of pain after 4 to 6 hours due to the weaning off the local anesthetic. Patients are asked to use ice and take anti-inflammatory medications or pain medications if needed.
Patients who undergo multilevel blocks or multiple bilateral blocks may feel weak after the procedure and may not able to ambulate for a few hours. Patients are followed up in the office and are usually put on physical therapy to stretch and strengthen the muscles of the back and the hip.
Selective nerve root block is different from an epidural injection as it blocks only the nerve root which are suspected to be causing the pain as compared to epidural injection which bathes all the nerve roots with the steroid injection and local anesthetic.
This is helpful not only being therapeutic, but also diagnostic to identify the specific level of pathology. At the same time, selective nerve root block has less complication rate as compared to an epidural injection.
Selective nerve root block delivers the steroid injection at the exact site where it needs to act. Systemic absorption of steroid is minimal. This is in comparison to oral steroids which effects all tissues of the body and may have detrimental effect of multiple organs.
Complications
Injection of the medication inadvertently to the adjoining structure like the blood vessel. Occasionally, the injection may become epidural and may cause numbing of multiple nerve roots. Rarely, process of injection will lead to bleeding into the area, which may compress over the nerve roots of the lumbar spine leading to cauda equina syndrome.
If the cauda equina syndrome happens then an emergent surgery may be needed to decompress the nerve roots.
Steroid injection may lead to increasing of blood sugar levels in next 2-3 days and therefore patients with Diabetes are asked to check their sugar levels frequently and consult their primary care if needed.
Prevention and Maintenance
Although selective nerve root blocks provide relief, they do not address the root cause of nerve compression. Therefore, ongoing physical therapy, exercise, and lifestyle modifications are recommended to strengthen the muscles around the spine and reduce the likelihood of further nerve irritation.
Proper posture, ergonomics, and weight management can also help prevent sciatica and reduce the need for repeated nerve root blocks or invasive interventions.
Research Spotlight
A recent study evaluated the efficacy of selective nerve root blocks (SNRB) in treating lumbar radiculopathy due to prolapsed intervertebral discs (PIVD).
In a cohort of 35 patients, SNRB significantly reduced pain and disability, with the mean Numeric Rating Scale (NRS) score dropping from 6.4 at baseline to 3.14 at 90 days, and the Oswestry Disability Index (ODI) improving from 14.31 to 6.86 over the same period. Additionally, the Straight-Leg Raise Test (SLRT) converted from positive to negative in all patients post-procedure, and only 11.4% had recurrence by 90 days.
These findings confirm that SNRB provides rapid and durable pain relief, serving as an effective non-surgical option for patients with radiculopathy from PIVD. This treatment can also be diagnostic, helping identify the exact level of nerve root compression (“Study on selective nerve root blocks for lumbar radiculopathy – See PubMed“).
Summary and Key Takeaways
Selective nerve root blocks are an effective treatment for radiculopathy and sciatica, particularly in patients with failed conservative treatment or those with multilevel spine issues. They provide both diagnostic and therapeutic benefits by pinpointing the level of nerve root compression and offering relief through steroid injections and local anesthesia.
While SNRBs are generally safe, proper imaging guidance and patient selection are key to ensuring a successful outcome. Patients experiencing persistent or recurrent radiculopathy despite conservative treatments may benefit from this procedure to improve mobility, reduce pain, and delay or avoid surgery.
Do you have more questions?
What is a selective nerve root block?
A selective nerve root block (SNRB) is a minimally invasive procedure where a local anesthetic and steroid are injected around a specific nerve root in the spine. This procedure is both diagnostic, helping to identify which nerve is causing pain, and therapeutic, providing relief from inflammation and pain.
How does an SNRB differ from an epidural steroid injection?
While an epidural steroid injection spreads medication over a larger area around the spine, an SNRB targets a single, specific nerve root. This makes it more accurate for diagnosing which nerve is responsible for your pain and helps to limit the spread of medication to nearby nerves.
How is the procedure performed?
After the skin is numbed with a local anesthetic, the doctor inserts a needle under fluoroscopy (X-ray) or CT guidance to ensure it reaches the correct nerve root. Once positioned, a contrast dye may be injected to confirm placement before administering the anesthetic and steroid.
How long does an SNRB procedure take?
The procedure itself usually takes about 15 to 30 minutes. Most of the time is spent positioning the needle correctly under imaging guidance.
. What conditions are treated with SNRBs?
SNRBs are commonly used to treat radicular pain from conditions such as herniated discs, spinal stenosis, sciatica, and post-surgical complications. They are also helpful in managing failed back surgery syndrome (FBSS) and radiculopathy due to osteophytes (bone spurs).
What can I expect after the procedure?
After an SNRB, you may experience immediate pain relief from the local anesthetic. However, it can take 2 to 3 days for the steroid to reduce inflammation and provide longer-lasting relief. Some soreness at the injection site is normal.
How is an SNRB different from surgery?
Unlike surgery, SNRBs are minimally invasive, don’t require anesthesia, and have a much shorter recovery time. They are often used as a diagnostic tool or to provide temporary relief while exploring non-surgical treatments. Surgery is typically reserved for cases where conservative treatments fail.
Will I need imaging before the procedure?
Yes, most patients will have undergone diagnostic imaging such as an MRI or CT scan to identify potential problem areas in the spine. This imaging helps guide the SNRB procedure by identifying which nerve root is likely causing the pain.
How is the pain from a nerve root different from muscle or joint pain?
Nerve root pain, or radicular pain, often radiates along the path of the nerve into the limbs. For example, nerve pain from the lumbar spine may travel down the leg (sciatica), whereas muscle or joint pain tends to be localized and doesn’t travel far from its source.
Are SNRBs painful?
Most patients tolerate SNRBs well. You may feel pressure or a mild ache during the procedure, but the area will be numbed with a local anesthetic to minimize discomfort. Some patients may experience brief pain as the needle approaches the nerve root.
Can SNRBs be used to treat sciatica?
Yes, SNRBs are commonly used to treat sciatica, which is caused by compression of the sciatic nerve in the lower back. The injection targets the affected nerve root to reduce inflammation and alleviate leg pain.
What is the role of imaging during the procedure?
Imaging, such as fluoroscopy or CT, is crucial for accurately guiding the needle to the targeted nerve root. This reduces the risk of complications and ensures the medication is delivered to the correct location.
What if the SNRB doesn’t work or provides only partial relief?
If an SNRB provides only partial relief or fails to alleviate your pain, it may suggest that multiple nerves are involved, or the pain is originating from another source. Your doctor may recommend additional diagnostic procedures, such as further nerve blocks or discography, to pinpoint the pain source.
The content on this page has been authored, edited, or approved by the doctors below, and was last reviewed for accuracy on December 5, 2025.
