A hip replacement is used to treat hip pain, by removing the hip joint and placing a artificial joint in it’s place. Most artificial hips last over 25 years. But no implant lasts forever. Over time, the moving parts slowly wear down, and tiny wear related particles can irritate the surrounding bone. This can cause the implant to lose its grip on the bone.
The technical term for this is aseptic loosening. When that happens, the old hip starts to hurt and feel unstable again. The treatment is a second surgery, called revision hip replacement. Here, the surgeon replaces the worn or loose parts with new ones.
This page explains why implants loosen, how doctors spot it, and what the repair surgery involves.
What happens when your hip replacement is worn out:
Here’s the basic idea of how it happens: your artificial hip is a metal or ceramic ball that glides inside a plastic-lined socket. Every step you take creates a tiny bit of friction, and over many years that produces microscopic particles.
Your body treats that debris like an irritant and reacts by slowly dissolving nearby bone. This is called osteolysis (breakdown of bone). As the bone around the implant thins out, the implant can work its way to become loose and start moving slightly. This causes pain and a feeling that the hip isn’t solid.
Some people’s implants wear faster than others. Things that speed it up include being younger or more active, carrying extra weight, having weaker bone, or having the original implant placed slightly off the ideal positioning.
The type of implant matters as well. Some material combinations create more debris than others.
When should you consider surgery:
The warning sign is pain that comes back after years of feeling a comfortable hip replacement. Pain is often felt in the groin and gets worse when you put weight on the leg or move around.
Some people also feel the hip slipping, clicking, or feeling unsteady. Most patients require revision/repeat surgery, as this process is not compatible with healing on its own. It tends to get worse with time.
If you notice this, it’s worth getting checked early. Doctors confirm what’s going on with a physical exam and imaging. This will usually include X-rays and may also get a CT scan or MRI. Usually we can see gaps or thinning around the implant if the process has been going on long enough.
We’ll also run blood tests and sometimes draw fluid from the joint to make sure an infection is not present. Sometimes an infection can present like this, but the treatment is very different. Diagnosing this early is important.
The longer this process is allowed to continue, the more bone you lose. This means that the revision surgery requires more dissection, more extensive metal implants, and use of additional strategies to deal with the bone loss. The more complicated the surgery, the higher the risks for complications afterwards.
What happens during surgery:
The repair is called revision surgery, and the goal is to remove the worn or loose parts and put in new, stable ones. Depending on what’s worn out, the surgeon might:
- Replace just one part: such as the loose stem in the thigh bone, or only the socket cup
- Replace the entire implant if both the ball-and-stem and the socket are critically involved.
Worn parts are taken out, any damaged or thinned bone is dealt with, and fresh components are fitted and anchored to the remaining healthy bone.
Newer implants often use longer-lasting plastic that resists wear better than older versions. This is a more complex operation than the first hip replacement. there’s less healthy bone to work with. It’s best done by a surgeon experienced in revisions.
Below is a image of an X-ray showing a worn out partial hip replacement, and the associated loose implant in the thigh bone. The breakdown of the bone surrounding the implant is visible. The image afterwards shown that removed implant.
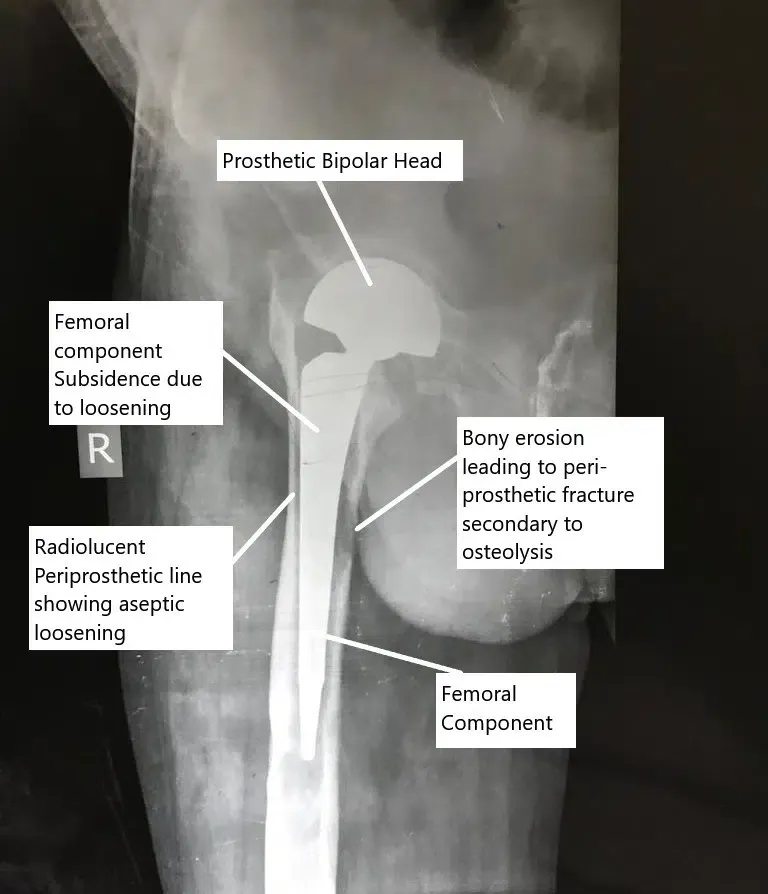
X-ray showing aseptic loosening of the hip replacement.
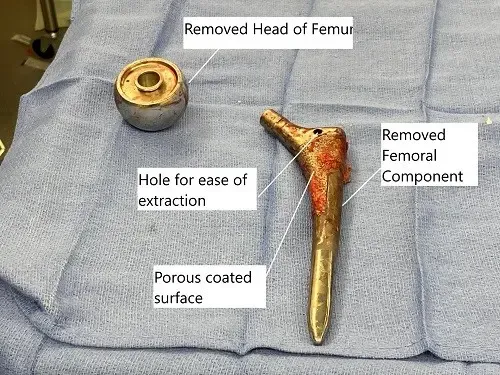
Extracted head of femur and the femoral component during revision surgery.
What does recovery look like:
Recovery from a revision is a lot like recovery from the first hip replacement, but it’s often a bit slower and more involved. This is because the surgeon is working with bone that has already been through one operation.
You can expect time on crutches / walker, physical therapy to rebuild strength and movement, and gradual return to your normal activities. Exact timelines vary a lot from person to person depending on how much bone was affected and how much of the implant had to be replaced.
Your surgeon will give you a plan based on your specific situation. As with the first time around, sticking to low-impact activities and avoiding high-impact ones like running and jumping helps the new parts last.
Most patients are up and walking the same day as the revision surgery. That is usually the goal. Most patients are walking with minor assistance at 6 weeks. By 3 months we usually expect most patient are back to their usual activities.
Major complications associated with revision surgery:
Revision surgery carries the same general risks as any hip replacement. However, it’s a more complex operation. This means that some of those risks are higher that a straight forward hip replacement. The main ones to know about:
- Infection: bacteria can infect the wound or deeper in the joint. This may require additional surgery if the infection penetrates deep into the joint.
- Blood clots: Clots in the leg can grow and travel to the lungs. This is dangerous, but we prescribe medicine and exercises to prevent it.
- Dislocation: This is when the new ball slips out of the socket. Typically it needs to be put back in, under sedation. It this happens repeatedly it can require more surgery.
- Bone-related problems: such as a fracture around the implant during surgery or trouble getting the new parts to anchor firmly, since there’s less healthy bone to hold them.
Your surgeon will go over how these apply to your case before you decide.
What if you don’t have surgery:
You don’t have to rush into a revision. Managing the symptoms for a while is reasonable in some cases. But a loose implant doesn’t tighten back up on its own.
Left alone, the slow bone loss around it tends to continue. This means more pain, more instability, and a hip that keeps getting harder to use.
There’s also a practical downside to waiting too long, the more bone you lose, the more complicated the eventual repair becomes. This makes it harder to get a great result. That’s why doctors recommend regular check-ups with imaging every few years after a hip replacement.
This way loosening can be caught and fixed before it does extensive damage. When to have the revision is a decision to make with your surgeon, based on your pain, your imaging, and how much the hip is affecting your daily life.
Do you have more questions?
How common is wearing out of a total hip replacement?
Wearing out of a total hip replacement is relatively common, especially in individuals who have had the implant for decades or are highly active.
Are there specific activities that increase the risk of wearing out a total hip replacement?
Activities that place repetitive stress on the hip joint, such as high-impact sports or heavy lifting, can increase the risk of wearing out a total hip replacement.
Can wearing out of a total hip replacement be prevented?
Wearing out of a total hip replacement cannot always be prevented but certain measures can help. This includes maintaining a healthy weight, avoiding excessive stress on the hip joint, and following care guidelines
What are the non operative treatment options for wearing out of a total hip replacement?
Treatment options may include conservative measures such as pain management, physical therapy, and activity modification, and the use of assistive devices (canes, walkers)
Can wearing out of a total hip replacement affect other parts of the body, such as the spine or knees?
Yes, wearing out of a total hip replacement can change the way you walk and place increased stress on other joints such as the spine or knees.
How often should individuals with a total hip replacement undergo follow-up appointments to monitor for signs of wearing out?
Individuals with a total hip replacement should undergo regular follow-up appointments with their orthopedic surgeon to monitor for signs of wearing out and assess implant integrity.
Can wearing out of a total hip replacement lead to complications such as metallosis or adverse tissue reactions?
Yes, wearing out of a total hip replacement can lead to complications such as metallosis (metal poisoning) or adverse tissue reactions due to the release of metal ions from the implant components.
Are there any dietary or lifestyle modifications that can help slow down the wearing out of a total hip replacement?
There are no specific dietary or lifestyle modifications proven to prevent wearing out of a total hip replacement. But, maintaining a healthy weight, staying physically active within recommended limits, and avoiding smoking may help optimize overall joint health.
Can individuals with a total hip replacement safely participate in physical activities such as sports or exercise classes?
In general, individuals with a total hip replacement can safely participate in low-impact activities such as swimming, cycling, or walking. However, high-impact sports or activities that place excessive stress on the hip joint. This can lead to early wear and the need for revision. However, many patient return to high impact activities after a hip replacement. It is a calculated risk, and dependents on what is important to you. It depends on what is important to you.
How does the type of implant material used in a total hip replacement affect the risk of wearing out?
The type of implant material used in a total hip replacement, such as metal-on-metal, metal-on-plastic, ceramic-on-ceramic, or ceramic-on-plastic, can impact the risk of wearing out and the longevity of the implant.
Can individuals with a total hip replacement experience symptoms of wearing out even if the implant appears intact on imaging studies?
Yes, individuals with a total hip replacement can experience symptoms of wearing out even if the implant appears intact on imaging studies. Wear-related changes may not always be visible on imaging and can manifest clinically. Often more advanced studies are needed to diagnose this
Are there any alternative treatments or therapies available for individuals experiencing symptoms of wearing out of a total hip replacement?
Alternative treatments or therapies for symptoms of wearing out of a total hip replacement may include non-invasive modalities such as acupuncture, chiropractic care, or physical therapy to manage pain and improve joint function. This does not address the root cause of the pain, but may help you cope with the pain.
Can wearing out of a total hip replacement affect the stability or alignment of the hip joint?
Yes, wearing out of a total hip replacement can lead to changes in implant position, joint stability, and alignment, which may contribute to symptoms such as pain, stiffness, and decreased mobility.
The content on this page has been authored, edited, or approved by the doctors below, and was last reviewed for accuracy on June 8, 2026.
