
Total Knee Replacement
Total knee replacement is a surgical procedure to replace the damaged parts of the knee joint with metal and plastic parts. It is one of the most common surgeries performed by orthopedic surgeons. Common causes for knee pain include arthritis caused by primary osteoarthritis, rheumatoid arthritis, psoriatic arthritis, and secondary arthritis. The surgery is performed when all conservative forms of management are exhausted.
Owing to the success of the surgery, a number of patients are today undergoing total knee replacement. By 2030, knee replacement surgery is projected to grow by 189 percent. Knee pain due to arthritis can be quite debilitating for patients of all age groups. Knee arthroplasty offers excellent pain relief with increased mobility.
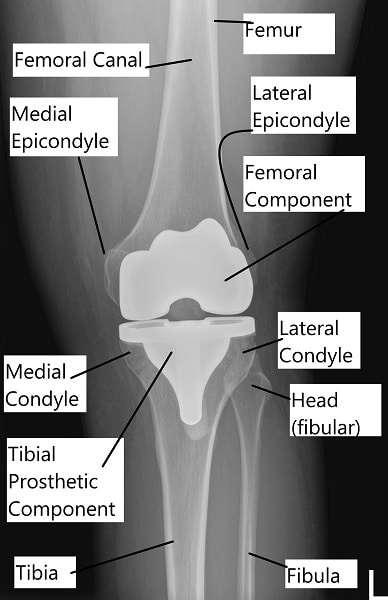
Total knee replacement X-ray
Anatomy
The knee joint is a large synovial hinge joint. The joint is formed by the lower end of the thigh bone (femur) and the upper part of the shinbone (tibia). The kneecap (patella) forms a joint with the lower part of the thigh bone.
Patella acts as a lever for straightening the leg. It also allows smooth gliding of the bones when straightening or bending the leg.
Articulating cartilage is a glistening white smooth tissue covering the end of the bones forming the joint. The cartilage also covers the undersurface of the patella. The cartilage is toughened and flexible to allow smooth gliding of the joint surfaces.
The ligaments surrounding the knee provide stability to the joint. The ligaments providing stability at the front and the back are anterior cruciate ligament and the posterior cruciate ligament. Medial and lateral collateral ligaments provide stability on the sides of the knee joint. Tear or laxity of the ligaments lead to instability and damage the joint.
Meniscus are small pads, one on the inner side and one on the outer side of the knee joint. Both the meniscus cushions the impact on the ends of the bones. They also provide additional stability to the joint. Both the meniscus and the ligaments have limited blood supply.
Synovium is a tissue lining the inner surface of the joint. The synovium secretes a watery thin, clear and sticky fluid known as synovial fluid. Just like machine oil, it acts as a lubricant allowing smooth gliding of the joint. Bursae are small fluid-filled sacs helping in smooth gliding of the structures around the knee joint.
Proper alignment between the femur and tibia is necessary for the distribution of joint forces equally. Muscles crossing the knee joint allow for bending and straightening the knee.
Causes
Arthritis due to variety of reasons remains the most common indication for total knee replacement. Various types of arthritis are primary osteoarthritis, secondary osteoarthritis, rheumatoid arthritis, or psoriatic arthritis.
With growing age, the structures which form the knee joint, including the bones, articular cartilage, tendons, ligaments, meniscus, and muscles degenerate. The changes culminate into tears of the meniscus and cartilage, leading to loss of smooth gliding of the joint. The joint may become inflamed and swollen.
Rheumatoid arthritis is a systemic disease often affecting multiple joints, especially the smaller joints. The knee joint may be affected as well and usually, both the knees may be involved. There is extensive destruction of the cartilage and subchondral bone with inflammation of the synovium. The destruction is carried out by the body’s immune cells recognizing the normal cells as foreign.
Other forms of arthritis such as psoriatic arthritis and gouty arthritis also lead to the destruction of the joint. Arthritis secondary to knee injury is known as secondary osteoarthritis. Injuries such as fractures or tears of the meniscus and ligament may cause incongruity of the joint surface. Young patients with a history of trauma to the injury may present with secondary arthritis.
Congenital or residual deformities while growing such bow legs or knock knees cause malalignment of the joint. The unequal distribution of forces leads to the development of early arthritis.
Symptoms & Management
Patients with advanced arthritis usually present with knee pain. The knee pain is especially aggravated on activities such as walking, squatting, bending, twisting or turning. They experience difficulty navigating stairs and report stiffness after periods of inactivity. Joint crepitus may be experienced which is described as a grinding/popping sensation on moving the knee.
A wide range of conservative management options is tried before knee replacement surgery. These include heat pads, physical therapist visits, weight loss, or glucosamine and chondroitin sulfate tablets. The patient may receive cortisone injections or visco-supplement injections in the knee.
Unfortunately, arthritis is a progressively worsening condition. The conservative management options may thin out and the pain may become more persistent. The patients who have exhausted all conservative treatment options are candidates for knee replacement.
Procedure
Before the procedure, the patients are examined thoroughly for any deformity in the knees. Their medical conditions are assessed for them to be medically fit to undergo the procedure. Routine blood tests and cardiograms are done as a part of presurgical testing. The surgery is usually performed either in general anesthesia or spinal anesthesia.
Cross-matching of the patients’ blood is done for blood transfusion if needed. Any kind of blood thinner is stopped a few days before the procedure. Imaging studies usually an X-ray and sometimes a CT scan may be done to assess the degree of bone loss. Preoperative planning is done to assess the correct biomechanical axis of the knees.
The joint is opened from the front and the damaged bone along with cartilage is removed. Bone cuts are made with specially designed jigs to prepare the joint surface. Both the anterior and posterior cruciate ligaments are usually sacrificed in posterior stabilized implants. The medial and lateral collateral ligaments are retained and surgically released to balance the alignment.
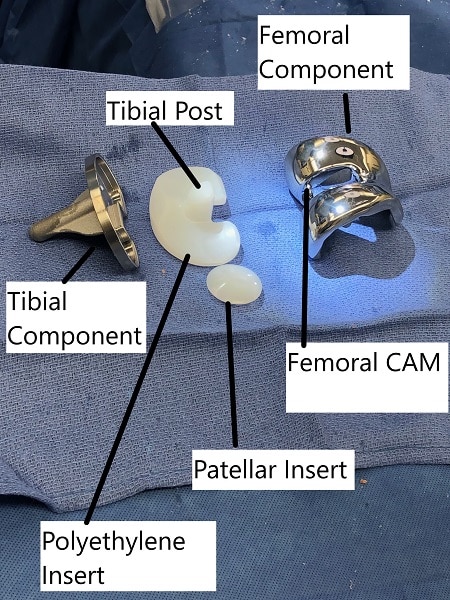
Prosthetic parts of total knee replacement
The metal parts are then introduced and are glued with acrylic bone cement. A special high-grade plastic (Polyethylene) is inserted between the metal parts acting as a stabilizer and cushion. The metal parts are made of a cobalt-chromium alloy and are designed to allow smooth gliding. The undersurface of the patella is resurfaced and a special plastic is cemented to the undersurface. The joint is thoroughly irrigated, cleaned and closed. Intraoperative medications may be injected to reduce post-op pain. The patient is shifted to the recovery room where their vitals are closely monitored.
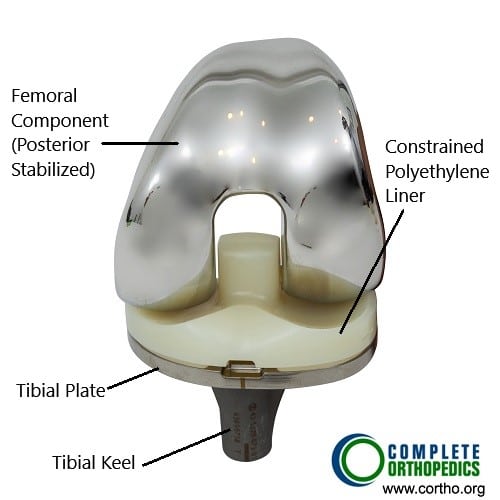
Total knee replacement components (front view)
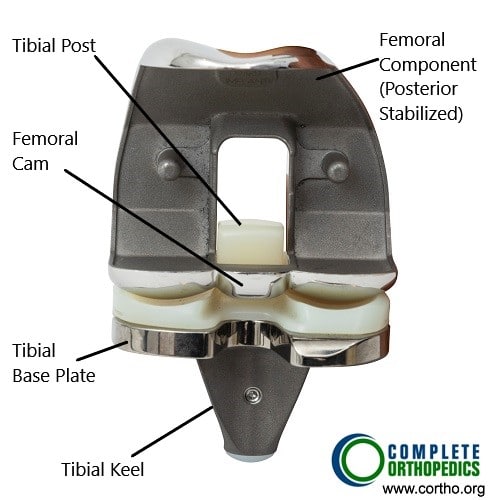
Total knee replacement components (back view)
The above images show the prosthetic knee replacement components from the front and the back. The femoral component (posterior stabilized) has a cam mechanism which allows posterior translation of the femur on the tibial post of the bearing surface. The femoral rollback aids in achieving deeper flexion which in a normal knee is done by the knee ligaments. The polyethylene insert is made of highly cross linked polyethylene, which is resistant to wear and tear. The keel of the tibial component is fixed in the upper part of the shin bone using bone cement.
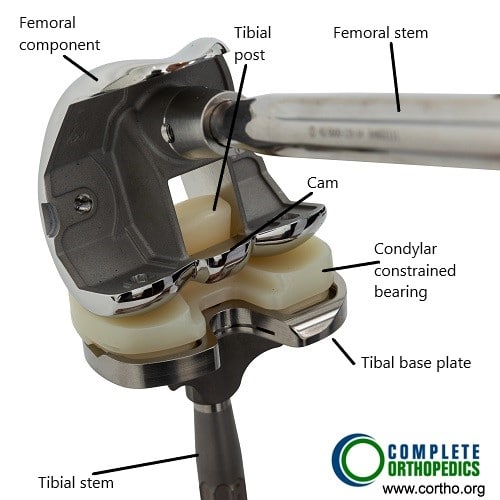
Revision knee modular components
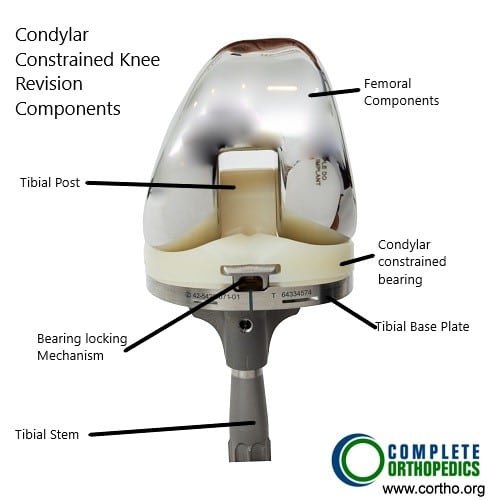
Revision knee modular components
The modular components shown in the images above are used in revision knee surgery or complex knee replacement. Depending upon the knee anatomy and bone loss, the surgeon is able to achieve greater stability of the prosthetic implant using modular components.
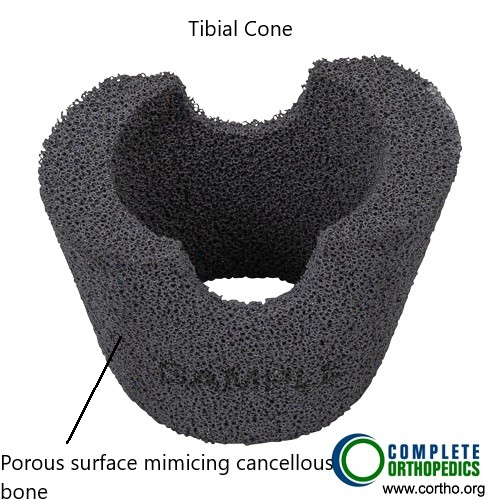
Tibial cone augment
Metal cone resembling trabecular bone may be used to fill in bone gaps encountered in the metaphyseal region intraoperatively. The trabecular surface pattern of the tibial cone ensures biological union of the component.
After the Procedure
The recovery time is expedited and patients are able to walk the same day of the procedure with support. The post-operative pain is managed with medications and usually, a blood thinner is prescribed to prevent blood clots. Physical therapy is initiated to regain strength and increase flexibility.
Most patients are able to go home the day after surgery. The patients are able to walk without support usually in 8-12 weeks. They are able to resume their daily activities. X-rays are taken of the artificial knee/replaced knee to check for proper alignment and fixation.
They are able to walk, climb stairs, bend, ride a bicycle, drive a car and climb stairs without any limitation. The patients are advised not to undergo any high impact activities such as running or jumping.
Possible complications
As true with any major surgery, they may be potential complications with a joint replacement surgery. There may be medical complications such as heart attack, stroke, or pneumonia. There may be intraoperative complications such as fractures, shortening, instability, nerve or blood vessel damage.
During the few weeks after the surgery, there is an increased risk of blood clots in the leg, infection or dislocation. In the following months, the patient may complain of persistent pain, a clunk while moving the knee, dislocation or stiffness. In the long run, there may be loosening of the implant or the plastic component may wear off.
Success
On average, a total knee replacement lasts for more than 15- 20 years, for some patients, it may last their lifetime. Owing to the success, total knee replacement surgeries are being performed regularly. The patients express satisfaction in being able to get back to their daily activities. They are pain-free and report greater range of motion.
References:
- https://aaos-annualmeeting-presskit.org/2018/research-news/sloan_tjr/

My name is Dr. Suhirad Khokhar, and am an orthopaedic surgeon. I completed my MBBS (Bachelor of Medicine & Bachelor of Surgery) at Govt. Medical College, Patiala, India.
I specialize in musculoskeletal disorders and their management, and have personally approved of and written this content.
My profile page has all of my educational information, work experience, and all the pages on this site that I've contributed to.