
Case Study: Right Total Knee Replacement with
Custom Instruments in a 67-year-old female
A 76-year-old female presented to our office with complaints of bilateral knee pain. She states the knee pain is especially worse in her right knee. She didn’t recall the exact onset of knee pain. She stated that the pain started 4-5 years ago.
The pain was mild in intensity when it first started but gradually progressed to severe in intensity. She had earlier received gel injections in both her knees but the initial relief didn’t last long. She also received cortisone knee injections with reported relief only for a week.
She also attended an outpatient physical therapy and some home exercise program. She feels that the pain worsened after some exercises she did at therapy. She feels relief with icing and rest. She takes Advil and Tylenol SOS for pain.
The pain was described as a dull ache located deep in the knee. There was no radiation of the pain. She complained of increased pain with activities such as walking, standing, getting up from a chair, negotiating stairs, bending, kneeling and turning.
She was a retired teacher and was quite distressed with her lifestyle limitation due to pain. She is unable to walk more than a block secondary to pain. He used a cane as an assistive device. She stated she took one step at a time to negotiate stairs and used banister.
She was a nonsmoker and denied any known drug allergies. She was currently taking Lipitor and Hydrochlorothiazide for hypercholesterolemia and hypertension. Both the medical conditions were well controlled with medications.
On physical examination, there was crepitus throughout the range of motion of both knees. There was tenderness on the right medial and lateral joint lines. There was tenderness on patellar facets. The range of motion of the right knee was from 10 degrees to 110 degrees. The left knee faired better with a range of motion of 0 degrees to 120 degrees.
The arch of motion of both knees was painful. There was no evidence of joint laxity or instability in all the planes. The examination of the bilateral hips and ankles was normal.
There was no distal neurological deficit. The bulk and tone of the bilateral lower extremities were normal. The bilateral lower extremity pulses were good volume. There was no bowel or bladder dysfunction.
Imaging studies revealed severe bilateral knee arthritis. The right knee was worse than the left side. She was advised right total knee replacement with custom instruments. Risks, benefits, and alternatives were discussed at length with her. She agreed with the plan.
As a part of the preparation of custom instruments, a preoperative MRI was done a few weeks prior to the procedure. Custom implants ensured less tissue trauma and accurate bone cuts for the procedure.


X-ray of the right knee in anteroposterior and lateral views.
OPERATION: Right total knee replacement.
IMPLANTS USED: Posterior stabilized 10 right standard femoral component right-sided with tibia F left cemented with 14 x 30 stem with poly 16 mm with a 32 x 8.5-mm diameter poly patella.
DESCRIPTION OF PROCEDURE: The patient was brought to the operating room after obtaining informed consent, signing the correct surgical site. The risks, benefits, and alternatives were extensively discussed with the patient prior to the procedure.
Anesthesia was obtained by the anesthesiologist. The patient was then definitely positioned, and the right knee was then draped and prepped in the usual sterile manner. A straight incision centered over the patella was used for the arthrotomy.
Skin and subcutaneous tissues were then incised. A medial parapatellar arthrotomy was then performed. The knee was then exposed and the femoral cutting guide was then placed into position. The distal cut was then performed. The anterior, posterior, and then the chamfer cuts were then performed.
Attention was then turned towards the tibia. The tibial cut was then performed. Lamina spreaders were used medially and laterally, and the remainder of the meniscus was then debrided. The notch cut was then performed and the femur was then placed into position followed by the tibia.
The tibia was then broached and the trial poly was then placed into position. The gap balancing was performed before the final broaching and was found to be correct. The patella was then resected. The drill holes were made in the patella and then the trial patella was then placed into position.
The knee was then reduced. The knee was then ranged through a full range of motion and the patellar tracking was found to be normal, and the gap balancing was then again checked and was found to be satisfactory.
The trial components were then removed. Thorough lavage was given. The femur was cemented into position. Excess cement was then removed. The tibia was then cemented into position. Excess cement was then removed. Poly was then placed over the tibia. The knee was then reduced.
The knee was then held in full extension and then the patella was cemented into position and held in position with a patellar clamp. The excess cement was removed after the cement hardened. The knee was injected with intraarticular injection and thorough lavage was given.
Medial parapatellar arthrotomy was closed with Ethibond, cutaneous tissues were closed with 0 Vicryl, subcuticular tissues were closed with 2-0 Vicryl, and skin was closed using staples. Sterile dressing was then applied, and the patient was then transferred to the postoperative care unit in stable condition.

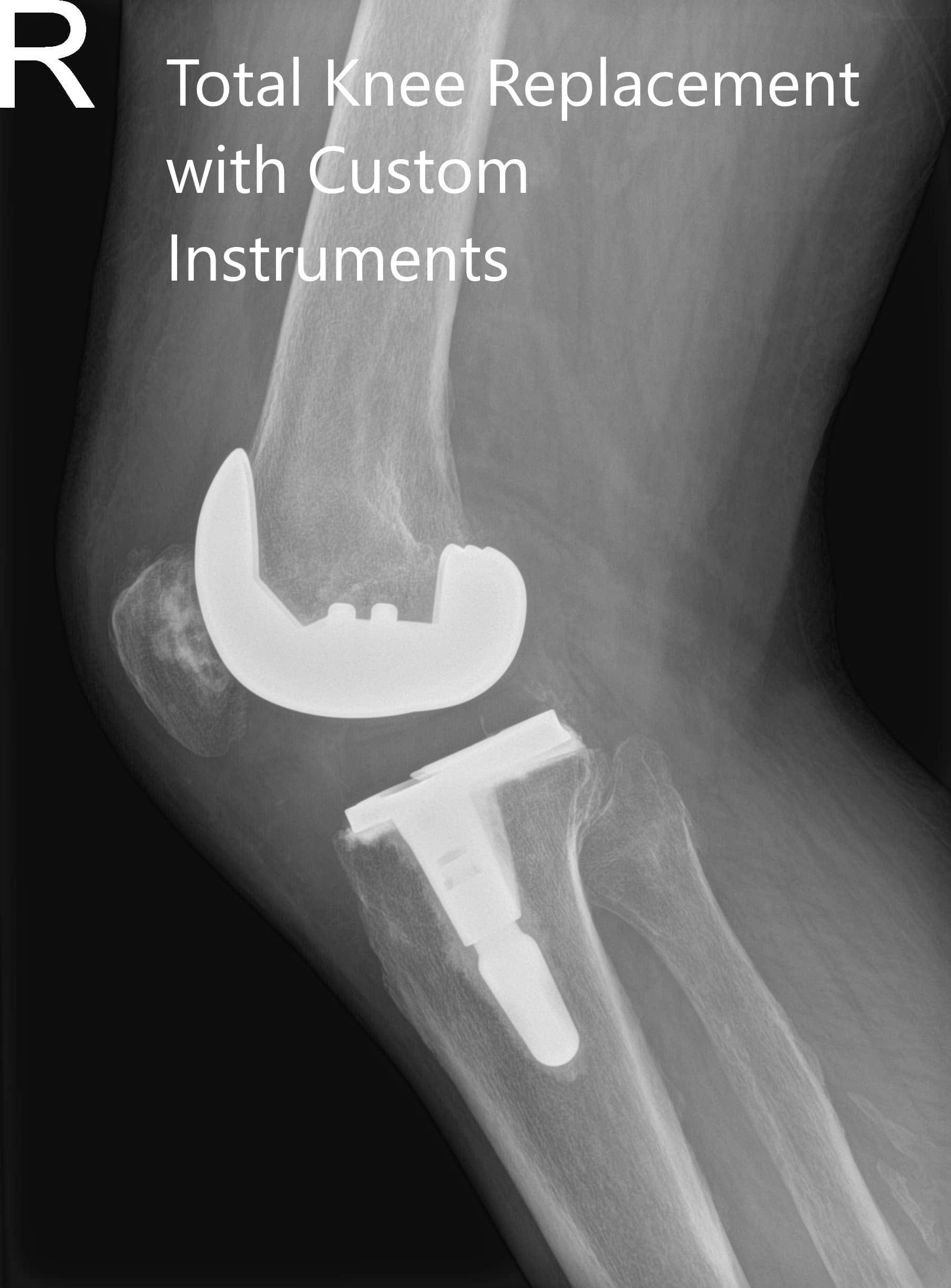
Postoperative X-ray of the right knee in anteroposterior and lateral views.
Post-op her recovery was expedited. She was standing and walking the same day of the surgery. Aspirin was given for deep vein thrombosis prophylaxis. The pain was managed with medications.
She started outpatient physical therapy to increase flexibility and improved range of motion. Two months post-op she demonstrated a full range of motion with zero pain. She was walking without an assistive device. She reported less pain in the left knee secondary to offloading of the weight. She was happy with the outcome of the procedure.
Disclaimer – Patient’s name, age, sex, dates, events have been changed or modified to protect patient privacy.

My name is Dr. Suhirad Khokhar, and am an orthopaedic surgeon. I completed my MBBS (Bachelor of Medicine & Bachelor of Surgery) at Govt. Medical College, Patiala, India.
I specialize in musculoskeletal disorders and their management, and have personally approved of and written this content.
My profile page has all of my educational information, work experience, and all the pages on this site that I've contributed to.